
Studies and data on trans women’s breast growth
Prepared for N. B. — March 15, 2017
Topics:
Anatomy Histology Timeframe Implants Antiandrogens Abnormalities Progestins
“Hormone Therapy in Adults: Suggested Revisions to the Sixth Version of the Standards of Care” (Feldman & Safer, 2009)
Anatomy Timeframe Progestins
p. 150:
In MtF patients, the following changes are expected to occur: increased breast hemicircumference (up to 12 cm), enlarged nipple and areole, decreased libido and erections, decreased testicular size.
p. 151:
Meyer et al. (1986) documented in a study of 60 MtF transgender persons followed prospectively that breast hemicircumference starts to increase by 2 to 3 months and reaches a plateau by 2 years.
p. 170:
Some clinicians believe progestins are necessary for full nipple development (Basson & Prior, 1998). However, a clinical comparison of feminization regimens with and without progestins found that the addition of progestins neither enhanced breast growth nor lowered serum levels of free testosterone (Meyer et al., 1986). . . . Clinicians are encouraged to review the evidence for efficacy, safety, and cost for various progestin agents, particularly for use as a second line agent to enhance breast development, while avoiding progestins in patients at high cardiovascular risk.
“Mammography and breast sonography in transsexual women” (Weyers et al., 2010)
Anatomy Timeframe Implants Abnormalities
[Note: 48 of 50 trans women in this study had breast implants. —ZJ]
p. 508:
In our centre, suppression of androgenic effects is achieved by the anti-androgen cyproterone acetate, while estrogen is the principal agent used to induce female characteristics. One of the desired effects of estrogen therapy is gradual growth of breast tissue. The latter effect is however highly variable, this is some patients will hardly develop some breast buds even after years of estrogen therapy while others have full breast development after 1–2 years.
p. 510:
In 11 patients the breasts were judged very dense (22%), in 19 (38%) “dense”, in 11 “slightly dense” (22%) while the remaining 9 (18%) were “translucent”. There was no correlation between the density of the breast tissue and estrogen levels ( p = 0.390).
p. 511:
Sonographic density was equally scored by the radiologist. In only 1 patient the breasts were very echodense (2%), 18 were judged “dense” and 18 “fatty” while the remaining 13 were “slightly dense”. There is a significant correlation between the density on mammography and on sonography. In 5 patients (10%) the retro-areolar ducts were visible on breast sonography, all of these ducts were ≤2 mm. In 5 patients (10%) cysts were present, all were <5 mm. There is no correlation between the presence of cysts and serum estradiol concentrations. In 5 patients abnormalities (other than small cysts) were visualized: 1 patient had a fibroadenoma, two had a lipoma, in 1 patient both prostheses were empty while in another rupture of one of the prostheses was suspected.



“Predictive Markers for Mammoplasty and a Comparison of Side Effect Profiles in Transwomen Taking Various Hormonal Regimens” (Seal et al., 2012)
Anatomy Timeframe Implants Antiandrogens
p. 4423:
The breasts of transsexual natal males taking estrogen therapy follow the same stages of development as are seen in natal female puberty (2). As such, it takes 2 yr of therapy to achieve maximum growth (2). Because the bony frame of the male chest differs greatly from the female, the resulting appearance of the thorax still differs from that of similarly developed natal females, often resulting in an appearance that is deemed unsatisfactory by patients, leading approximately 60% to request an augmentation mammoplasty (3).
p. 4424:
A baseline hormone screen was taken before any hormonal therapy was taken. There was no difference in hormone levels between the augmentation and control groups on the baseline hormone screen (see Table 2). However, when subjects are categorized according to whether they self-medicated (see Table 2), the estradiol level was significantly higher at baseline in those who self-medicated and went on to require breast augmentation as compared with controls (216.75 ± 73.22 vs. 78.33 ± 14.43 pmol/liter, P = 0.02). The testosterone levels of those in the self-medicating group who also required subsequent breast augmentation were higher, but this did not reach statistical significance (18.37 ± 14.01 vs. 4.08 ± 2.92 nmol/liter).
p. 4425–4426:
These data appear to show that those people who self-medicate with estrogen are more likely to be referred for breast augmentation surgery than those who do not. The duration of estrogen exposure and the duration of estrogen use before attending the GIC (and any subsequent mammoplasties) resonate with the initial finding that self-medication is associated with greater need for breast augmentation. This is consistent with studies on puberty induction in natal girls in whom rapid estrogen exposure was found to lead to premature breast bud fusion and poor breast development (8). Those transwomen who self-medicate with estrogen may be taking too large a dose at initiation to promote appropriate subsequent breast growth, resulting in a poorer final breast outcome. As breast hemicircumference was not measured in this study; it was not possible to determine whether individuals who underwent breast augmentation had objectively smaller breasts. It should be noted, however, that unlike the situation in natal women, breast hemicircumference measurements are limited in their ability to quantify the appearance of breast development in transwomen. The median breast development in transwomen is reported to be 19 cm, which is near natal female norms (2). Despite this fact, 60% of transwomen still present for breast augmentation.
p. 4426:
The use of spironolactone as an antiandrogen seemed also to be associated with an increased incidence of breast augmentation in transwomen. The other, more specific antiandrogens and GnRH analogs were not. Spironolactone is a mineralocorticoid receptor antagonist that acts as an androgen receptor partial antagonist as well as an estrogen receptor agonist. As such, in addition to blocking the androgen receptor (which is its primary purpose in this situation), it also has a significant estrogenic action at the doses used in transwomen. One can postulate that this could lead to an excessive estrogenic action and consequent poorer breast outcome by the same mechanism as that seen when patients self-medicate with estrogens. It is interesting that the other antiandrogens, cyproterone acetate and finasteride, do not appear to be used more frequently in those requiring breast augmentation compared with controls, suggesting that this is not a class effect of antiandrogens.



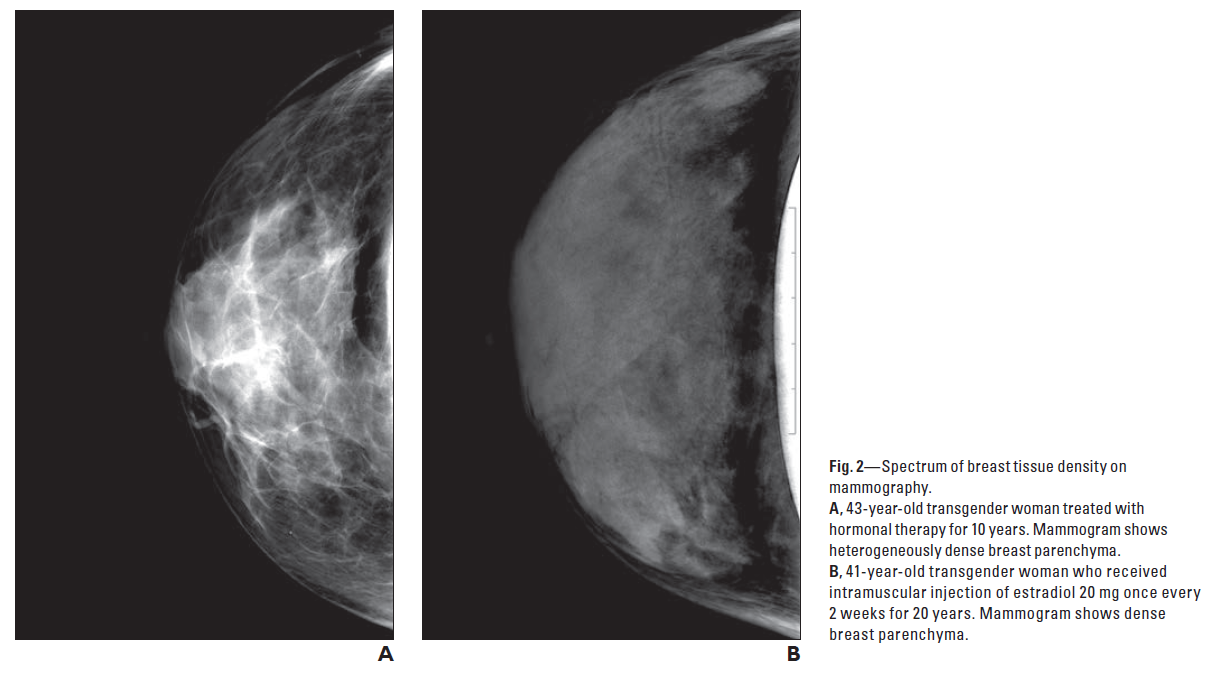
“Patient Satisfaction with Breasts and Psychosocial, Sexual, and Physical Well-Being after Breast Augmentation in Male-to-Female Transsexuals” (Weigert et al., 2013)
Anatomy Implants


“Clinical Review: Breast Development in Trans Women Receiving Cross-Sex Hormones” (Wierckx, Gooren, & T’Sjoen, 2014)
Anatomy Histology Timeframe Antiandrogens Progestins
p. 1242–1243:
Meyer et al. [17] investigated breast growth in 52 trans women during cross-sex hormone treatment. Notably, 41 trans women received cross-sex hormone treatment with a median of 26.4 months before inclusion in the study. Different estrogen regimes (ethinyl estradiol [EE], conjugated estrogen, or both) were analyzed, and 15 trans women of their sample (28%) additionally received a progestational agent. No difference in breast size was observed between trans women who received progestogens compared with the others. . . .
The authors observed that the increase in breast size usually begins within 2–3 months after the start of cross-sex hormone treatment and progresses over 2 years. Final breast size was not different in relation to which type of estrogen had been used (conjugated estrogens or EE) or to the dose of EE. The latter was in contrast with their previous cross-sectional study in 38 trans women whose breast size, measured by the maximal breast tissue circumference, differed according to the dose of estrogen therapy: trans women using EE 0.05 mg daily and those using conjugated equine estrogens 5 mg daily had a higher maximal breast circumference compared with respectively those using EE 0.01 mg daily and those using conjugated equine estrogens 1–2.5 mg daily [16]. Orentrich et al. [15] neither found a clear association between final breast size and dose of estrogen in four case reports. Seal et al. [13] neither observed a difference in type of estrogen treatment between trans women who underwent augmentation mammoplasty compared with those who did not.
p. 1243:
Kanhai et al. [20] investigated the effect of cross-sex hormone therapy, consisting of cyproterone acetate 100 mg (an anti-androgen with progestational properties) and EE 100 μg daily, on thorax circumference at the nipple. They observed that the circumference at the nipple increased from a mean of 91–93 cm during the first 18 months of cross-sex hormone treatment.
p. 1243:
In the study of Dittrich et al. [22], 60 trans women were treated with GnRH analogs and estradiol valerate 6 mg daily. Seventy percent of them wished to undergo augmentation mammoplasty as they found their breast size too small after 24 months of hormonal therapy. Only 35 percent of trans women in their group had a B cup (mean difference of 14–16 cm between circumference at the nipple and circumference just below the breast) or more, 35% had an A cup (mean difference of 12–14 cm), and 30% had less than an A cup after 2 years of cross-sex hormone therapy. The authors concluded that this treatment regime, not including a drug with progestational properties, had a similar efficacy compared with prior reported treatment regimes using cyproterone acetate and EE [21] and thus questioned the use of progestogens as part of the endocrine treatment of trans persons in order to enhance breast growth.
p. 1243:
Prior et al. [18] also observed that most trans women developed an A cup. They explored the effects of 12-month administration of spironolactone 100–200 mg in combination with conjugated equine estrogen 0.625 daily up to 5 g daily on feminization in 50 trans women. In spite of this modest breast development, few trans women in their group sought augmentation surgery afterwards. Reutrakul and colleagues as well as Sosa and colleagues reported that all trans women developed tanner stage 2 or 3, unless they underwent augmentation mammoplasty [19,24].
p. 1244:
Limited data are currently available on predictors of breast size. Meyer et al. [17] found that duration of hormonal therapy influences final breast size. Some authors suggest that depending on the age of trans women, other effects are to be expected and that breast growth in young trans women may be more pronounced compared with older women [25]. Additionally, individual breast tissue sensitivity and body weight are suggested as important determinants of breast size in trans women [15,32–34], although to our knowledge, these hypotheses are only experience based. In trans women, shoulder width may also be an important factor of perceived breast size and configuration [13].
p. 1244:
Overall, these findings may suggest that besides estrogen levels, the degree of testosterone suppression may also be an important factor regarding breast development in trans women. Androgen levels have indeed been found to inhibit breast tissue proliferation in vitro [35–37] in rodents [38] and monkeys [39,40]. However, in human clinical studies, the results are inconclusive as most [41,42] but not all studies [43,44] observed that higher total testosterone levels are associated with increased breast tissue proliferation in both pre and postmenopausal women.
p. 1244:
The hypothesis that excessive estrogenic action negatively affects breast development brings up the question whether a step-up dose of estrogens would be preferable to enhance breast development in trans women. To our knowledge, no data are available on the effects of this treatment on breast development of trans women. However, step-up dosages of unopposed estrogens are usually prescribed for puberty induction (e.g., in Turner girls). This therapy is mainly prescribed to avoid acceleration of bone maturity by high-dose estrogen treatment resulting in a reduced final height. However, beneficial effects on breast development have been suggested, although clinical rather than experience based [47].
p. 1244–1245:
The available evidence does not provide support for better effects on breast size of adding progestogens to cross-sex hormone administration in trans women as suggested by some authors [14,18,48–51]. However, it should be said that the quality and amount of available evidence are extremely poor and hamper any firm conclusion at this moment. . . . Furthermore, all progestogens by definition have some progestational activity, but they differ in chemical structure, metabolism, pharmacokinetics, affinity, potency, and efficacy via steroid receptors and intracellular action. All these differences can translate into very different biological and clinical effects and advocate the absence of a class effect of progestogens [54].
p. 1245:
The central role of estradiol in initiating breast growth at puberty is revealed by the poordeveloped breast of estrogen receptor-alpha knockout mice [55], whereas progesterone knockout mice showed to have a morphologically indistinguishable ductal architecture from wild-type virgin mice [56]. Moreover, during pubertal induction in girls, early administration of progesterone is not recommended as premature initiation of progestin therapy can compromise ultimate breast growth [57].
p. 1245:
It is however of note that progesterone is known to be an important determinant of the histology of the breast in cis women. When the mammary epithelial of the progesterone knockout mouse is transplanted into a wild-type parous mouse, the obligatory role of progesterone in acinar and lobular development is demonstrated [58,59]. Additionally, other theoretical advantages of progesterone administration might be the fact that breast epithelium exhibits maximal proliferation in the luteal phase of menstruation, when progesterone levels are at their highest [60] and increased mammographic breast density is observed when progestogens are administered [61]. However, importantly, there is no evidence that these histological and mammographic differences result in clinically significant breast size differences.
“Breast Imaging in the Transgender Patient” (Phillips, 2014)
Anatomy Histology Timeframe Abnormalities
p. 1150:
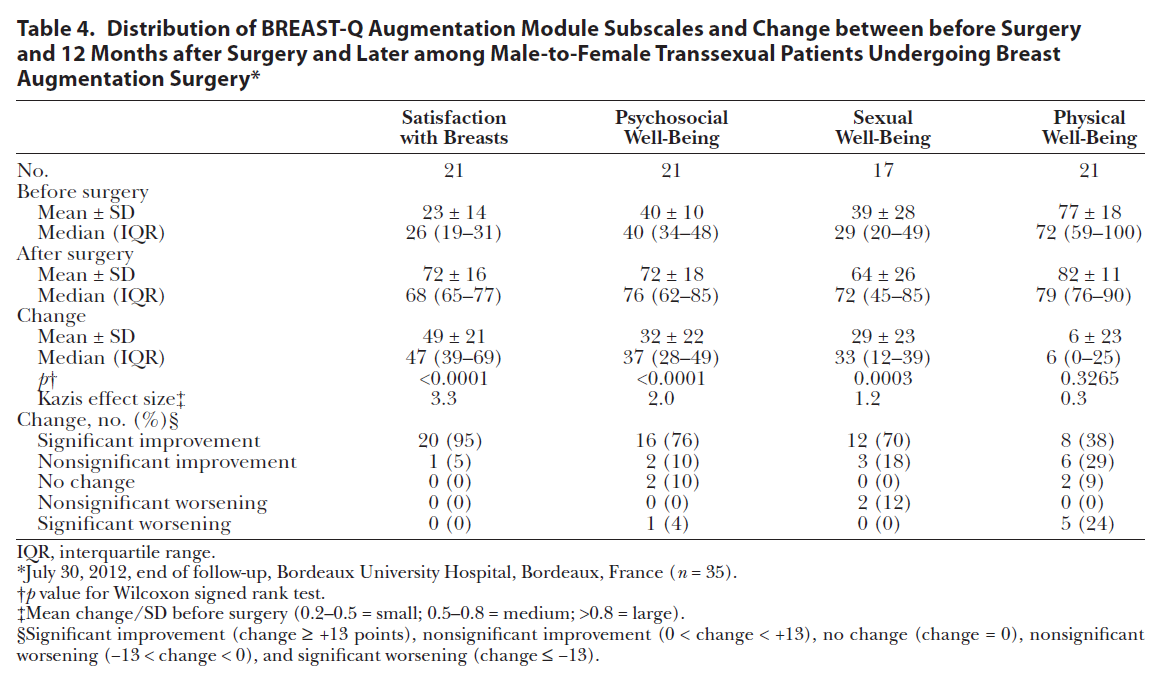
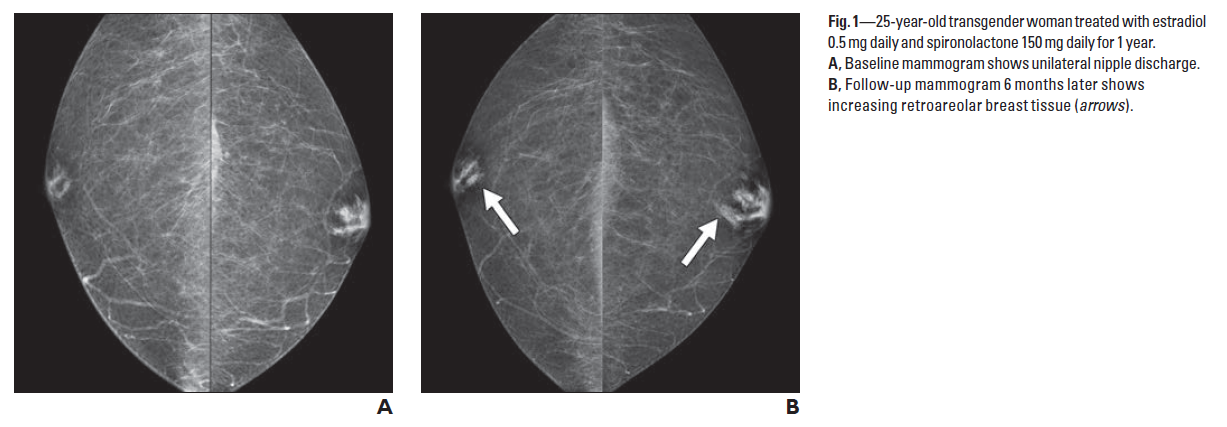
There are expected physiologic changes that occur in the breasts of a transgender woman after taking hormonal therapy that should not be viewed as pathologic, nor do they warrant additional imaging. Breast tissue will increase over time, reaching maturity by 2–3 years with a more pronounced nipple-areola complex [2] (Fig. 1). Transgender women can develop a spectrum of breast tissue density including heterogeneously dense and extremely dense breast tissue (Fig. 2). The breast tissue that develops should not be referred to as gynecomastia. One study has shown that this tissue more closely resembles breast tissue seen in natal women because it contains lobules [15]. These changes may be associated with clear bilateral nonspontaneous nipple discharge. If the discharge is unilateral, bloody, or spontaneous, further evaluation may be necessary to exclude other pathology. Diagnostic evaluation of nipple discharge should begin with ultrasound if the patient is younger than 30 years old.
p. 1151:
It is important to recognize that as breast tissue begins to develop, there may be lobule formation similar to that occurring in natal women. Therefore, entities typically not seen in natal men, such as cysts (Fig. 5) and fibroadenoma, can develop [21, 22]. To our knowledge, there are no published studies discussing the appearance of fibroadenoma in this population, but we have seen two cases at our institution of fibroadenoma in transgender women, which, as one might expect, have a similar imaging appearance to fibroadenoma seen in natal women’s breasts (Fig. 6).
“Breast Care in the Transgender Individual” (Maycock & Kennedy, 2014)
Anatomy Histology Timeframe Abnormalities
p. 76:
Breast and nipple-areolar development is rarely as complete in MtF individuals on hormone supplementation as it is in genetic females and Tanner stage 5 is rarely reached. In the first 3 to 6 months of therapy, tender breast buds begin to form, and maximum development is usually achieved after 18 to 24 months of hormone therapy and is permanent. Male-to-female individuals may choose to consider augmentation after 2 years if they are unsatisfied with their breast growth. Weight gain in thin transgender women may also add to breast volume.
p. 76:
However, because administration of estrogen causes the genetically male breast to develop the acini and lobules of a female breast, the anatomy may become indistinguishable and therefore place MtF persons at risk for developing fibroadenomas. There have been 2 documented reports of fibroadenomas in the MtF population.
###