
The anti-trans advocacy group Society for Evidence-based Gender Medicine (SEGM), a prominent hub of career expert witnesses and commentators against gender-affirming medical care, will meet in New York City on October 9-12, 2023 for a conference featuring several leaders in the “evidence-based medicine” (EBM) movement, according to a flier obtained by Gender Analysis. The contents of the document are consistent with an October 10 “International Perspectives Conference” advertised on Eventbrite by SEGM.
The flier reveals several previously unknown connections and ongoing projects of SEGM members, including several not previously known to be affiliated with SEGM:
- Evgenia “Zhenya” Abbruzzese, a serial entrepreneur and coauthor of numerous commentaries with SEGM director Julia Mason and Florida anti-trans expert witness Stephen Levine (Levine et al., 2022; Abbruzzese et al., 2023), is now acknowledged in the flier as a cofounder of SEGM.
- Abbruzzese holds a 2019 patent (US10431109B2) on a browser-based tool to block web sites and searches related to “medically unexplained symptoms”, which she says “may be caused by anxiety, stress, or other mental health disorders”; she claims that people with these symptoms “unwittingly engage in symptom-amplifying behavior and thoughts”. Fellow SEGM conference presenter Lisa Littman asserted in 2018 that “online advice promotes the idea that nonspecific symptoms should be considered to be gender dysphoria” (Littman, 2018), allegedly creating an online “social contagion” of gender dysphoria that she parallels with the “deviancy training” of pro-eating disorder content. With this patent, Abbruzzese conceivably stands to gain from the implementation of policy frameworks such as the Kids Online Safety Act, which Sen. Marsha Blackburn (R-TN) claims is necessary for “protecting minor children from the transgender” on social media, and the Heritage Foundation’s Project 2025, which considers “propagation of transgender ideology” to be “pornography” that should be blocked from the internet entirely.
- Sallie Baxendale, an epilepsy expert who was present at SEGM’s April 24, 2022 meeting with the U.S. Department of Health and Human Services while listing her affiliation as “self”, is now described as having “contributed to the Cass review” of youth gender-affirming care in England; she also “recently completed a systematic review of the impact of puberty blockers on cognitive development in adolescence”.
- Although Baxendale has extensively praised the Cass review at Unherd, the British Psychological Society, and the BMJ (Bell et al., 2022), she does not appear to have publicly disclosed her involvement in the review.
- Kathleen (“Dr. Kate”) Goonan, a healthcare executive and “advisory and advocacy specialist” for the anti-trans group Genspect, is described as currently volunteering at Massachusetts General Hospital as a “parent advocate with health care providers and schools”.
- Goonan previously appeared as a panelist at a March 23, 2023 Moms for Liberty/Heritage Foundation event on “Exposing Gender Ideology”, speaking with Jay W. Richards of the creationist Discovery Institute and Erin Brewer of Advocates Protecting Children/Partners for Ethical Care. During the panel, Richards described “introducing children to these concepts in gender ideology” as “grooming”, and argued: “That’s why the word ‘grooming’ is important even when the teacher is not a pedophile.”
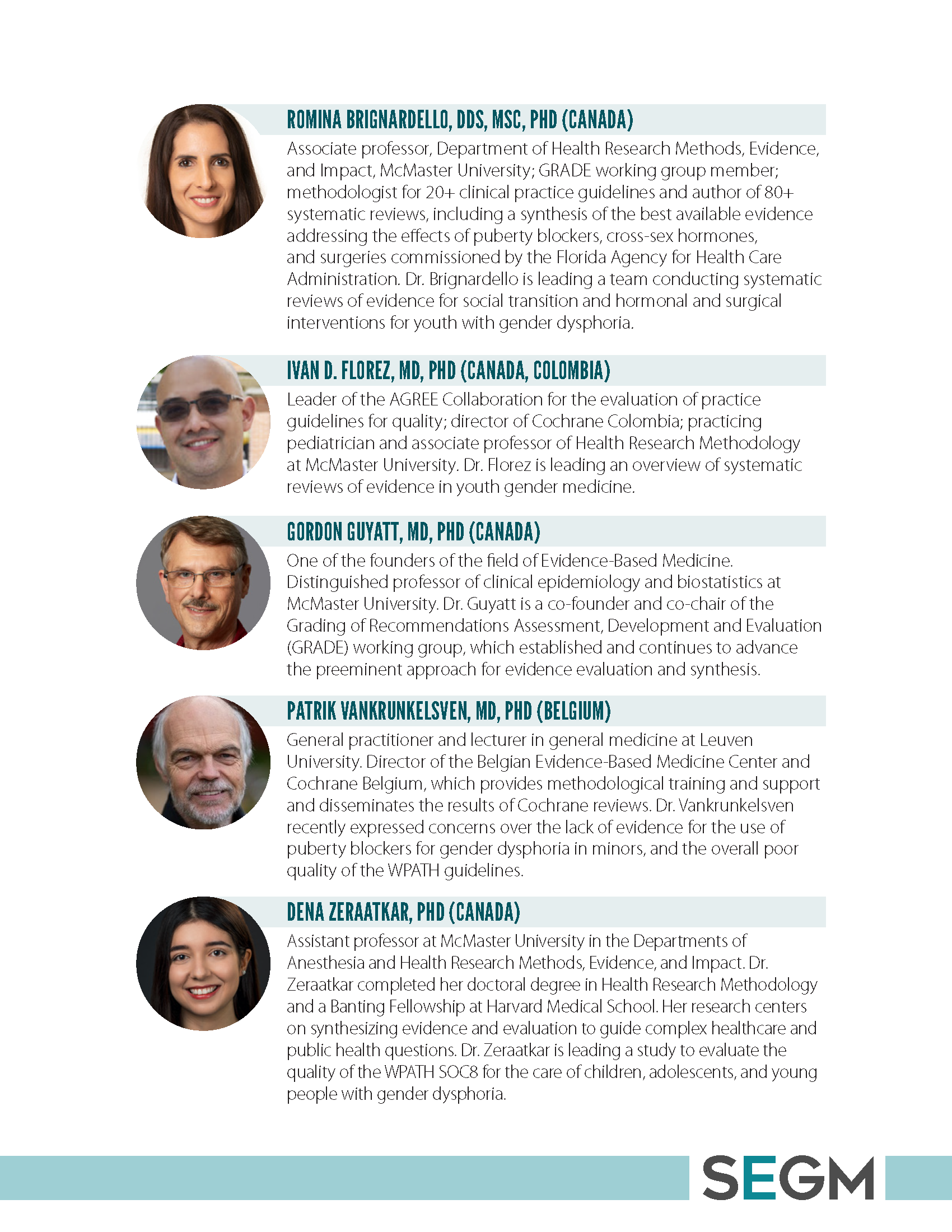
- Romina Brignardello-Petersen, author of a Florida-commissioned “overview of systematic reviews” of gender-affirming care to support the state’s predetermined outcome of “Care Effectively Banned”, is currently “leading a team conducting systematic reviews of evidence for social transition and hormonal and surgical interventions for youth with gender dysphoria”.
- Riittakerttu Kaltiala, a state-invited witness for Florida’s trans youth care ban and leader of Finland’s Tampere University youth gender clinic, is described in the flier as being “currently involved in two major international evidence review projects in the field of gender medicine.”
- Florida Board of Medicine appointee Patrick K. Hunter, a member of SEGM and the anti-trans Catholic Medical Association, stated in Brandt v. Rutledge (ECF no. 69-6, May 1 2022) that he had lectured with Kaltiala in Finland.
- Anne Wæhre, a child and adolescent psychiatrist in Norway, has “recently spent a year as a Research Fellow in Pediatrics at Boston Children’s Hospital”, a facility that received months of bomb threats in 2022 targeting its youth gender clinic program.
- Wæhre coauthored a 2018 op-ed in Aftenposten arguing that transmasculine adolescents should not receive gender-affirming care, concluding: “keep treatment-eager sexologists on a short leash, they are buying/giving beards and deep voices to the nation’s daughters, left we have lost fertility and an uncertain future” (Krumsvik, 2019).
- Ivan D. Florez, director of the evidence synthesis group Cochrane Colombia and leader of the core EBM group AGREE Collaboration (see Yao et al., 2020), is currently “leading an overview of systematic reviews of evidence in youth gender medicine”.
- Dena Zeraatkar, an assistant professor at the McMaster University Department of Health Research Methods, Evidence, and Impact (HEI), is now “leading a study to evaluate the quality of the WPATH SOC8 for the care of children, adolescents, and young people with gender dysphoria”.
The following images are taken from the 16-page flier:












These newly revealed connections represent a significant evolution of SEGM from its origins as a crypto-Catholic fringe group, to an increasingly entrenched threat harnessing the global prestige of the EBM movement and its leadership, which constitutes a currently dominant “methods regime” (Littoz-Monnet & Uribe, 2023). EBM is not to be confused with the overall use of evidence and observation in science and medicine (Worrall, 2007), as this recently emergent and misleadingly branded movement advocates for a highly structured yet highly restrictive approach to evidence synthesis: evaluating (and discarding) relevant scientific literature by rote classification of study design, while dismissing subject matter experts and experienced clinicians as sources of “bias”. Rather than critically examining and synthesizing a variety of quantitative and qualitative evidence, this approach replaces that challenge with the apparent simplicity of checklist-like processes that strongly devalue any evidence not obtained in randomized controlled trials (Balshem et al., 2011).

The accessibility of these nonspecific methods, with no need for EBM-trained methodologists to possess content expertise on the topics before applying an approach that “screens out about 98% or more of the medical research literature as not being ready for clinical use” (Haynes, 2002), has increasingly allowed these methods experts to supplant subject experts in determining recommendations for the clinical treatment of patients. Sallie Baxendale contends that this “evidence-based” approach “should be as uncontroversial as motherhood and apple pie”. In practice, the turn toward EBM has presented a variety of new challenges:
- Randomized controlled trials attempt to use balancing to eliminate all confounders including those that are unknown, ideally providing an unbiased estimate of the average effect of a treatment, whereas non-randomized observational studies can only account for confounders that are known (Deaton & Cartwright, 2018). For this reason, EBM’s leading evidence rating system, GRADE, assumes RCTs are of an overall higher quality than observational studies (Siemieniuk & Guyatt, 2017).
- At the same time, RCTs of a particular treatment may not have been conducted, and various designs of observational studies may be the best evidence available; a 2014 Cochrane review even concluded that “on average, there is little evidence for significant effect estimate differences between observational studies and RCTs”. RCTs may not always be possible: it can be unethical to withhold a treatment from a control group when it has already been observed as likely to be effective for their conditions, as in the case of puberty pausers for trans adolescents. They can also be impractical, as seen in the case of puberty pausers for cis youth with central precocious puberty: in Mul et al. (2001), every subject allocated to the control group ultimately dropped out in order to receive the treatment outside of the trial.
- RCTs can be valuable for measuring the outcome of one-time interventions for an acute condition, but can be an inadequate design for studying complex interventions, primary prevention in public health, and dynamic conditions that have a chronic course (Krauss, 2018; Reddon et al., 2020). When applied in clinical practice, the average treatment effect observed in an RCT is used for reference class forecasting of the expected result for a patient given the treatment; this assumption of generalizability is undermined when the patients in an RCT sample are not representative of the treated population overall, often due to strict eligibility criteria that exclude patients who have co-occurring conditions or are taking multiple medications (Kennedy-Martin et al., 2015; Van Spall et al., 2007).
- Systematic reviews of a narrowly defined clinical question are conducted via a standardized and transparent process, with thorough documentation of the terms used in comprehensive searches of the largest databases of clinical literature, enabling others to perform replications of the review and see the reasons why each study was included or excluded (Koffel & Rethlefsen, 2016). EBM regards systematic reviews as occupying top position in a “hierarchy of evidence” along with randomized controlled trials (Murad et al., 2016). The GRADE approach, an expert consensus of methods, provides a largely deterministic set of instructions for methodologists to rate the quality of studies; higher-quality evidence is considered to be of greater certainty that its conclusions reflect the true effect of an intervention (Murad, 2017). GRADE uses these levels of evidence to determine whether clinical practice guidelines should make strong or weak recommendations, a binary that “provides clear direction to patients, clinicians, and policy makers” (Guyatt et al., 2008).
- Because the content of a systematic review is dependent upon the search strategy, this means that different choices by researchers or variations in their competence at constructing searches can produce low-quality systematic reviews (Uttley et al., 2023); the fact that a review is systematic is not a guarantee of high quality (Greenhalgh et al., 2018). However, this perception created an incentive for the proliferation of highly repetitive systematic reviews of poor quality during the first 18 months of the COVID-19 pandemic (Pearson, 2021). The involvement of a clinical librarian or search specialist is associated with more effective search strategies, but many systematic review teams do not include a librarian (Koffel, 2015).
- Although systematic reviews are intended to achieve greater objectivity and reproducibility in summarizing medical evidence on a topic, authors must still make subjective judgments when rating the strength of evidence in several domains, and reviewers often disagree on these ratings (Berkman et al., 2013). A different team of reviewers replicating the systematic review may come to different conclusions. And while GRADE specifies narrow criteria for making strong recommendations based on “low-quality” (non-RCT) evidence, in practice, up to 50% of clinical practice guidelines still contain “discordant” strong recommendations based on evidence that does not meet these criteria (Chong et al., 2023). Ultimately, the rise of systematic reviews has recapitulated the problem they were meant to solve: originally serving as a distillation of essential clinical evidence after ‘screening out 98% or more of the literature’, systematic reviews are increasingly bundled into overviews of systematic reviews (McKenzie & Brennan, 2017), and practitioners of EBM methodology are now told that they “shouldn’t read (most) systematic reviews” (Rada, 2017).
With support from key individuals in this tightly connected cluster of methodology groups – including Gordon Guyatt, Ivan D. Florez, Romina Brignardello-Petersen, the GRADE Working Group (GWG), AGREE Collaboration, the World Health Organization Guidelines Review Committee (GRC), national branches of the Cochrane Collaboration, and the McMaster University HEI – SEGM now has access to a potentially limitless pipeline of apparently credible expert methodologists, trained to testify that gender-affirming care is supported by only “low quality” evidence or is “not evidence-based” on the grounds that this evidence does not include randomized controlled trials of transitioning.
Gender Analysis forecasts that EBM leaders’ cooperation with SEGM will substantially increase the challenge of credibly countering these arguments in policymaking and litigation, and may substantially increase the time it will take to restore previous levels of access to gender-affirming care in SEGM-affected countries. We recommend that the trans community and our advocates learn the established practices of the EBM approach to evidence appraisal and clinical recommendations, study the history of the EBM movement’s emergence and the regulatory organizations that have adopted its principles, and familiarize themselves with the ongoing clinical and methodological debate over EBM’s fundamental limitations and its observed shortcomings in real-world settings. It is essential to understand these practices and their rationale before engaging in informed criticism of their potential misuses in a variety of clinical contexts – an ongoing issue which is not limited to transgender medicine. We intend to issue a collection of “EBM readers” highlighting a wide range of essential sources on these topics and their relevance to the trans community and access to gender-affirming care.
List of sessions at the SEGM October 9-12 International Perspectives Conference
Pre-conference session, Monday, October 9, 3:00 – 7:00 PM
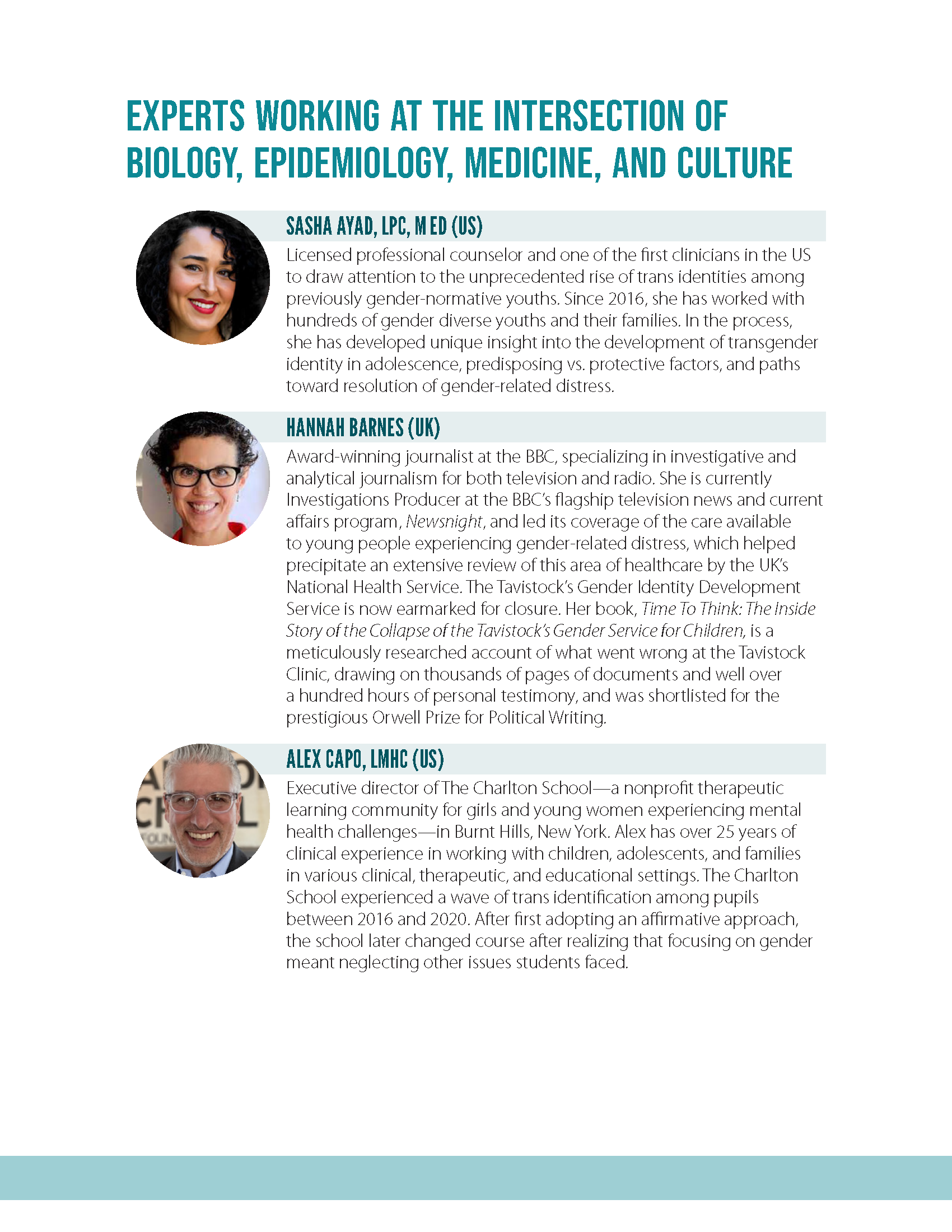
- The “gender clinic model of care”: Hannah Barnes, Jamie Reed, Anna Hutchinson
- Social and culture factors and youth identity formation
- Foundational research behind gender-affirming care
- Evidence-based medicine primer
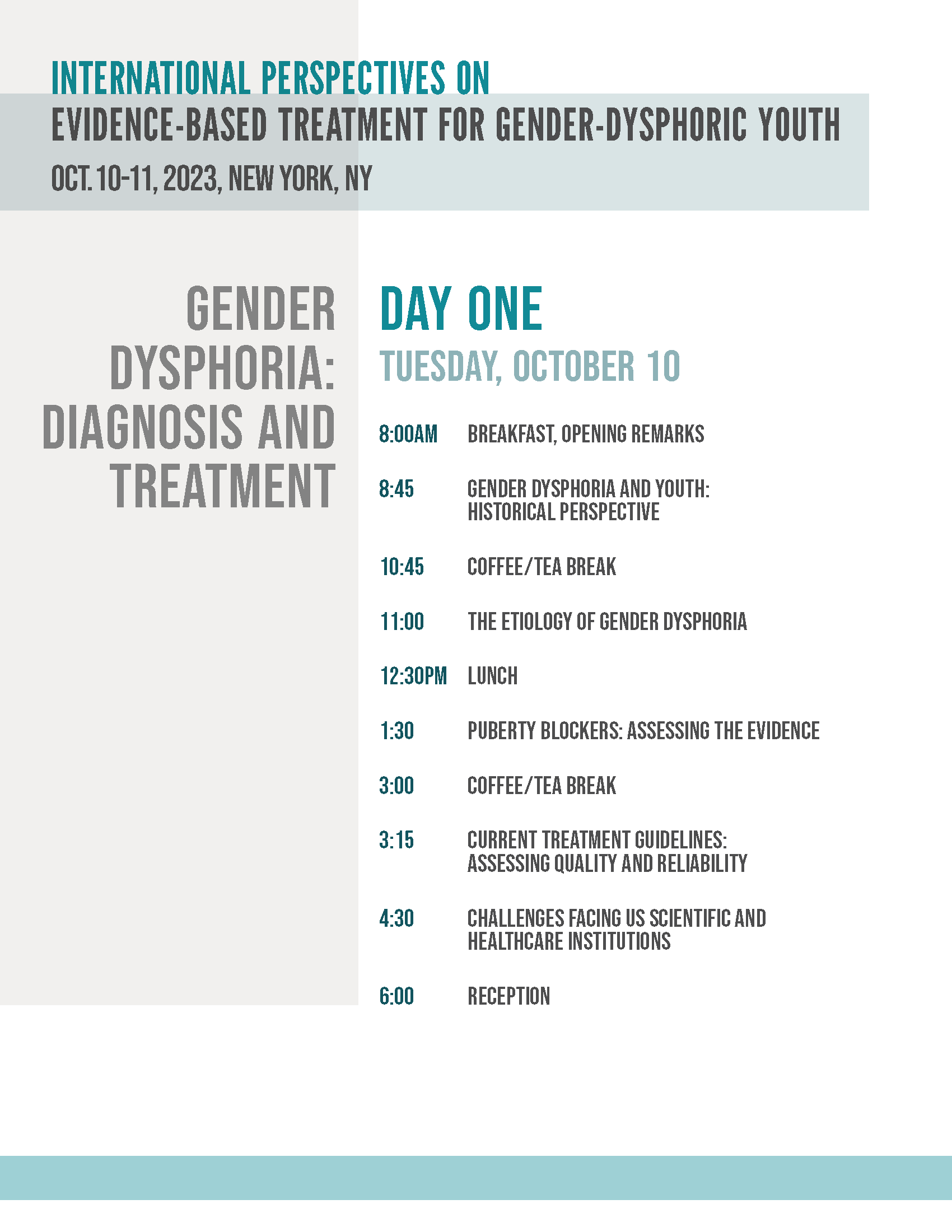
Day one, Tuesday, October 10 – Gender Dysphoria: Diagnosis and Treatment
- Gender dysphoria and youth: Historical perspective (8:45 AM)
- The etiology of gender dysphoria (11:00 AM)
- Puberty blockers: Assessing the evidence (1:30 PM)
- Current treatment guidelines: Assessing quality and reliability (3:15 PM)
- Challenges facing US scientific and healthcare institutions (4:30 PM)
- Reception (6:00 PM)
Day two, Wednesday, October 11 – Bridging the Evidence Divide
- Breakfast, participant reflections (8:00 AM)
- Lessons from the largest youth gender clinic in the world with Hannah Barnes (8:45 AM)
- The growing chasm between European and US approaches (9:15 AM)
- Aligning gender medicine with the evidence: A conversation with the founder of evidence-based medicine, Gordon Guyatt, MD (11:00 AM)
- Social transition: Assessing the evidence and impact (2:00 PM)
- Creating credible treatment guidelines based on systematic reviews of evidence: The evidence-based path forward (3:45 PM)
- Closing remarks (5:00 PM)
Post-conference session, Thursday, October 12, 9:00 AM – 12:00 PM
- Psychosocial approaches to managing gender dysphoria
- Advocating for evidence-based solutions within medical societies
- Q&A / Next steps discussions
List of speakers at the 2023 SEGM conference
- Zhenya Abbruzzese (SEGM cofounder; principal of J Curve Consulting; manager at Cambia Health Solutions; founder of Enigma Health)
- Erica Anderson (former USPATH president; former WPATH board member; expert affidavit in B.F. v. Kettle Moraine; amicus brief in appeal of Parents v. Montgomery County Board of Education)
- Sasha Ayad (Wider Lens Consulting; Gender: A Wider Lens; Inspired Teen Therapy; board member of Institute for Comprehensive Gender Dysphoria Research)
- Hannah Barnes (BBC Newsnight)
- Sallie Baxendale (University College London Institute of Neurology)
- Susan Bewley (King’s College London Department of Women and Children’s Health)
- Michael Biggs (Sex Matters board member; expert report in Dekker v. Weida)
- Romina Brignardello-Petersen (GRADE Working Group; McMaster University HEI)
- Alex Capo (The Charlton School, Burnt Hills, NY)
- Alison Clayton (University of Melbourne School of Historical and Philosophical Studies)
- Roberto D’Angelo (SEGM president; ICGDR treasurer)
- Laura Edwards-Leeper
- Ivan D. Florez (McMaster University HEI; leader of AGREE Collaboration; director of Cochrane Colombia)
- Paul Garcia-Ryan (Gender Exploratory Therapy Association; Open Therapy Institute)
- Kathleen Goonan (Genspect advisory and advocacy specialist)
- Moti Gorin
- Gordon Guyatt (GRADE Working Group; McMaster University HEI)
- Anna Hutchinson (Integrated Psychology Clinic; Explore Consultation; ICGDR board member)
- Kristopher Kaliebe (expert declaration, expert report, and rebuttal expert report in Dekker v. Weida; expert declaration in K.C. v. Individual Members of the Medical Licensing Board of Indiana)
- Riittakerttu Kaltiala (Tampere University Hospital Department of Adolescent Psychiatry)
- Mikael Landén
- Stephen Levine (GETA guidelines coauthor; DELR LLC; expert affidavit in B.F. v. Kettle Moraine; contributor to a previous rejected Cochrane systematic review of puberty pausers)
- Lisa Littman (ICGDR president)
- Julia Mason (SEGM board member)
- Carrie Mendoza (director of FAIR in Medicine)
- Jamie Reed
- Leor Sapir (Manhattan Institute)
- Patrik Vankrunkelsven (director of Cochrane Belgium and CEBAM)
- Samuel Veissière (Ubisoft Montreal)
- Anne Wæhre (Oslo University Hospital Department of Pediatrics)
- Dena Zeraatkar (McMaster University HEI)
- Ken Zucker
If you appreciate Gender Analysis, you can support our work on Ko-Fi or Patreon!


