
Commentary on: The Observer, “The Observer view on gender dysphoria: criminalising therapy poses risk to children’s welfare” (2023-10-22)
Summary
- In a recent editorial, The Observer argued that bans on conversion practices in the UK should encompass anti-gay but not anti-trans conversion therapy, on the grounds that “the fluidity of gender dysphoria makes it a completely different phenomenon to sexual orientation in young people”.
- Anti-gay conversion activists do not recognize such a distinction, uniformly consider anti-trans conversion practices to fall within the scope of their anti-gay practices, and have historically made the same arguments in favor of allowing anti-gay conversion therapy – assertions irresponsibly echoed by The Observer in opposing a ban on anti-trans conversion practices.
- These parallel arguments are made by the most prominent anti-gay conversion groups currently active in the UK and abroad, and include the following claims: sexuality in youth and young adults is fluid; most youth who identify as gay will not do so in adulthood; this alleged sexual fluidity should be explored in therapy to identify “underlying causes” of being gay; gay affirmative psychotherapy and bans on anti-gay conversion practices are purely “ideological” and not “evidence-based”; and bans on these conversion practices endanger the health and welfare of the public. The UK’s leading anti-gay conversion groups have consistently made these assertions in defense of conversion practices throughout the past five years.
- Anti-gay and anti-trans conversion activists both seek to portray queer and trans identities as fleeting phenomena, merely transient youthful confusion superimposed on an underlying cisgender heterosexuality. In reality, the vast majority of trans and gender-diverse youth exhibit long-term stability in their gender identities, and are frequently aware of their transness for several years before ever disclosing this to an adult.
- These conversion practices are not severable: they consist of the same substance, and can only be usefully understood as anti-LGBTQ conversion practices altogether. Regrettably, The Observer has thrown its weight behind the very same claims used by anti-gay conversion activists to promote these dangerous practices. In this case and elsewhere, transphobia is simply a recycled form of homophobia.
In its October 22 editorial, The Observer praised NHS England for abandoning a gender-affirming model of therapy for trans and gender-questioning youth, and embracing a supposedly “more evidence-based approach”. This approach would treat even social transition as a rare and exceptional case, instead offering “talking therapy that includes exploration of the reasons for their gender distress” – reasons allegedly including “autism, childhood trauma, children grappling with their own developing same-sex attraction, and intense discomfort about puberty”.
The authors lament that this non-affirming “exploratory therapy” could be derailed by a possible ban on anti-LGBTQ conversion practices, arguing that gender dysphoria has “fluidity” while sexual orientation does not:
There are a number of serious challenges for the NHS in rolling out a new approach; the underfunding of child mental health services and some clinicians’ continuing ideological affinity to the affirmative model. Another is that campaigners are seeking to make the provision of exploratory therapy effectively impossible by ensnaring it in an ill-defined criminal ban on trans “conversion therapy”. The ban has been linked to parallel proposals to ban gay conversion therapy; yet the fluidity of gender dysphoria makes it a completely different phenomenon to sexual orientation in young people.
However, The Observer fails to acknowledge that this appeal to fluidity is a near-universal argument made by anti-gay conversion activists for decades. Just as in the case of anti-trans conversion therapy, anti-gay conversion activists have extensively promoted “fluidity exploration in therapy”, offered psychodynamic explanations for being gay, attributed homosexuality to childhood upbringing and trauma, and even argued that most gay people will “desist” from being gay by the age of 25.
The same arguments for anti-gay conversion are now aimed at trans youth and adults, by some of the same individuals working for the same fringe anti-LGBTQ groups, including the International Federation for Therapeutic and Counselling Choice, Alliance for Therapeutic Choice and Scientific Integrity, Core Issues Trust, and the American College of Pediatricians. These groups are not historical relics, but active organizations promoting anti-gay conversion in the UK and US within the last decade, and they do not regard anti-trans conversion as being in a class apart from their anti-gay efforts. In recent years, leaders of these groups have recently served as experts facilitating restrictions on gender-affirming medical treatment in Florida and other Republican-controlled states.
Their assault on LGBTQ identities is a battle on all fronts for our community: there is no “LGB without the T” on this issue. The Observer has falsely framed transgender identities as uniquely unstable, when nearly all trans youth report being aware of their gender for years before coming out and are consistent in their gender after coming out; meanwhile, non-affirming parents in private anti-trans “support groups” have often admitted that their child has identified as trans for five years or more. For these reasons, anti-trans conversion practices are correctly recognized as falling under the same definitions of conversion therapy as anti-gay practices.
Conversion practices have been defined, and non-affirming therapy is an anti-trans conversion practice
The Observer asserts that “[n]o one has been able to precisely define what ‘trans conversion therapy’ is”, claiming that this would be “an impossible-to-define ban”. Yet the authors immediately offer one such definition:
But advocates for a ban clearly envisage it including therapy to explore the causes of a child’s gender distress and help them feel more comfortable in their body as an alternative to medicalisation.
They go on to describe this hypothetical ban as “criminalising exploratory conversations between a therapist and a young person that could be perceived as denying their identity”. The examples given by The Observer do appear to constitute conduct that would be encompassed by mainstream definitions of conversion practices. The American Academy of Child and Adolescent Psychiatry’s 2018 policy statement defines conversion therapy as follows:
“Conversion therapies” (or “reparative therapies”) are interventions purported to alter same-sex attractions or an individual’s gender expression with the specific aim to promote heterosexuality as a preferable outcome. Similarly, for youth whose gender identity is incongruent with their sex anatomy, efforts to change their core gender identity have also been described and more recently subsumed under the conversion therapy rubric. These interventions are provided under the false premise that homosexuality and gender diverse identities are pathological.
A report to the United Nations Human Rights Council in 2020 (A/HRC/44/53) offered a similar definition:
“Conversion therapy” is used as an umbrella term to describe interventions of a wide-ranging nature, all of which are premised on the belief that a person’s sexual orientation and gender identity, including gender expression, can and should be changed or suppressed when they do not fall under what other actors in a given setting and time perceive as the desirable norm, in particular when the person is lesbian, gay, bisexual, trans or gender diverse. Such practices are therefore consistently aimed at effecting a change from non-heterosexual to heterosexual and from trans or gender diverse to cisgender.
The US Substance Abuse and Mental Health Services Administration (2023) has also defined conversion practices in “Moving Beyond Change Efforts”, specifically highlighting non-affirming anti-trans “exploratory therapy” as an example of such a practice:
SOGI change efforts, commonly referred to as “conversion therapy” or “reparative therapy,” are practices that aim to suppress or alter an individual’s sexual orientation or gender to align with heterosexual orientation, cisgender identity, and/or stereotypical gender expression. SOGI change efforts are premised on or motivated by the belief that diversity in sexual orientation and/or gender identity and expression is a deficit, mental illness, or pathology. … This includes approaches that discourage youth from identifying as transgender or gender-diverse and/or from expressing their gender identity. Sometimes these are misleadingly referred to as “exploratory therapy.”
Finally, the state of Queensland, Australia (2022) has provided detailed examples of conversion practices, including “counselling to … not affirm their orientation, attraction or gender identity and expression”:
These practices are based on the disproven and dangerous ideology that being LGBTQA+ is a disorder or involves deviant behaviour that requires correction or suppression. … The most common examples of conversion practices include counselling to:
suggest that a legitimate aim of therapy might be to change or suppress sexual orientation or gender identity and expression;
encourage a person to abstain from sex or relationships;
encourage a person to ‘de-transition’ or not affirm their orientation, attraction or gender identity and expression;
dehumanise and shame a person because of their sexual orientation or gender identity or expression;
coerce gender-conforming behaviours;
attempt to create a causal relationship in a person’s mind between early childhood experiences and their sexual orientation or gender identity and expression.
The Observer is incorrect that conversion practices have not been defined, and likely correct that contemporary anti-trans “exploratory therapy” would be prohibited by bans on conversion therapy, given the prevailing accepted definitions of conversion practices. In some places, they are already prohibited: members of the anti-trans Society for Evidence-Based Gender Medicine (SEGM) have stated that their ability to provide gender non-affirming therapy, including “gender exploratory” practices, is limited by laws against conversion practices in certain US states and several Australian states, including Queensland (Deposition of Dianna Kenny, 2023-05-30). Not only is it possible to define and ban anti-trans conversion practices, it has already been done elsewhere.
The arguments for anti-gay and anti-trans conversion practices are broadly identical, including appeals to “fluidity”
UK-based conversion advocacy groups
The International Federation for Therapeutic and Counselling Choice (IFTCC), registered as a company in the UK in 2017 after hosting conferences internationally in 2015 and 2016, is a leader in activism for anti-gay and anti-trans conversion practices. At IFTCC’s London launch event in October 2018, the group issued a statement against banning conversion practices for queer people “who wish to explore with a therapist the fluidity of their same-sex attractions and behaviours in the context of determining their heterosexual potential.” In their statement, IFTCC claims to advocate for “patients’ self-determination should they desire to pursue their potential for fluidity and change in unwanted-same sex attractions and behaviour.” The document was coauthored by leaders of three groups endorsing anti-gay conversion practices: Michael R. Davidson of UK’s Core Issue Trust (CIT), Carys Moseley of UK’s Christian Concern, and Christopher H. Rosik of the US-based Alliance for Therapeutic Choice and Scientific Integrity (ATCSI) (formerly the National Association for Research and Therapy of Homosexuality, NARTH).
Also in 2018, CIT published “A Response to the UK Government’s Proposed Ban on ‘Conversion Therapy’”, explicitly linking exploration of “fluidity” in anti-gay and anti-trans conversion therapies and endorsing both as a combined practice:
In supporting calls for this a ban, the UK Government is hampering the rights and freedoms of individuals who seek alternatives to gay-affirming therapies who wish to explore the fluidity of their sexual attractions, their heterosexual potential or to overcome their gender confusion.
Similarly, Rosik announced in 2016 that ATCSI had voted to give their anti-gay conversion practices the absurd and misleading name of “Sexual Attraction Fluidity Exploration in Therapy (SAFE-T)”:
By stressing therapeutic exploration, the new term accurately conveys that the therapist is not being coercive but merely assisting individuals in a client-centered examination of their sexual attractions. … Scientifically, the fluidity of sexual orientation (and, for our purposes, especially same-sex attractions) for many women and men is now beyond question (Diamond & Rosky, 2016; Katz-Wise, 2015; Katz-Wise & Hyde, 2015).
IFTCC’s September 2022 “International Declaration on ‘Conversion Therapy’ and Therapeutic Choice” continues to describe same-sex desire as “overwhelmingly fluid”, and even calls those who no longer have same-sex partners “desisters”:
In particular, Natsal-3 showed approximately 2.9% were sexually active with the same sex or both – but another 2.9% had desisted same-sex sex five or more years ago (S2 Table). Most of these desisters were sexually active with the opposite sex and identified as heterosexual. … SSA [same-sex attraction] is not a mirror image of OSA [opposite-sex attraction]. For the respective populations involved, OSA is overwhelmingly fixed. SSA is overwhelmingly fluid and most often comes with opposite sex attraction too. Persons with both-sex attractions commonly experience fluidity in sexual attraction feelings and behaviour.
Like The Observer, IFTCC depicts conversion practices as mere “therapy conversations” and “exploration”:
LGBT activists in governments and elsewhere conflate the ill-defined term ‘CT’ (including morally reprehensible and historically abandoned aversion techniques) with standard (predominantly psychodynamic, evidence-based) therapy conversations, explorations of fluid sexual attractions and pastoral conversations where individuals harmonise the wholeness of their religious and sexual selves.
And similar to The Observer, IFTCC goes on to object that “conversion therapy” is itself an “ill-defined ideologically inspired phrase”. This declaration was cosigned by Core Issues Trust, Christian Concern, ATCSI, American College of Pediatricians (ACPEDS), Christian Medical & Dental Associations (CMDA), UK’s Fair Cop, Andre Van Mol (of ACPEDS and CMDA), and Quentin Van Meter (of ACPEDS). Van Mol had previously given a presentation at IFTCC’s 2020 conference, and Van Meter serves on IFTCC’s board.
North American conversion advocacy
The US-based American College of Pediatricians, and leading members like Quentin Van Meter, Andre Van Mol, and Michelle Cretella, have also played a leading role in disseminating arguments appealing to sexual “fluidity” to defend anti-gay conversion practices. In a March 2010 letter listing Quentin Van Meter and Michelle Cretella as serving on the board of directors, ACPEDS claimed that “most” queer adolescents would be effectively heterosexual “by age 25”:
Rigorous studies demonstrate that most adolescents who initially experience same-sex attraction, or are sexually confused, no longer experience such attractions by age 25. In one study, as many as 26% of 12-year-olds reported being uncertain of their sexual orientation, yet only 2-3% of adults actually identify themselves as homosexual. Therefore, the majority of sexually-questioning youth ultimately adopt a heterosexual identity.
The letter’s attached factsheet offers a familiar statistic that’s more recently been cited in claims that most trans youth will “desist” from being trans, while asserting that “therapy for the trauma” is needed to address homosexuality:
Most students (over 85%) with same-sex attractions will ultimately adopt a heterosexual orientation if not otherwise encouraged. Most questioning students are experiencing temporary sexual confusion or are involved in experimentation. … For many youth, homosexual attraction develops due to negative or traumatic experiences, such as sexual abuse. These students need therapy for the trauma, not affirmation of a “gay identity”.
This echoes the priorities of newer anti-trans groups such as Genspect, whose vice director Alasdair Gunn has privately called to “focus relentlessly on the problem of transition for under 25s”. Laura A. Haynes, a member of IFTCC and ATCSI and a consultant to ACPEDS, argued in 2022 for Missouri to ban gender-affirming medical treatment for anyone under the age of 25.
Making the connection between anti-gay and anti-trans conversion practices even more explicit, ACPEDS’ Cretella argued in June 2014 that “treatment” of youth’s gender dysphoria (formerly gender identity disorder) was necessary to prevent same-sex desire:
The emotional suffering of these children is indisputable and many homosexuality affirmative researchers agree that GID is treatable. Up to 75% of untreated gender discordant boys and one to two thirds of untreated discordant girls will develop SSA. On the other hand, SSA may be prevented when GID is treated successfully.
In support of this claim, Cretella cites controversial youth gender clinicians Ken Zucker and Susan Bradley’s 1995 book “Gender Identity Disorder and Psychosexual Problems in Children and Adolescents”. Zucker recently spoke at the anti-trans group SEGM’s October 2023 “International Perspectives Conference”, while Bradley went on to endorse the 2020 anti-trans “School Resource Guide” by the Child & Parental Rights Campaign alongside endorsements by Quentin Van Meter, Andre Van Mol, and Laura A. Haynes. In a 1985 book chapter, Bradley proposed that queer sexuality and transgender identity in youth are both caused by “increased sensitivity and poor anxiety tolerance”, and recommended “discouraging homosexual experience”:
With the gender-disturbed early adolescent, efforts to diminish cross-sex mannerisms and social-skill training to allow better integration with same-sex peers seems critical. For many adolescents and their families, the key issue is whether one can or should change what appears to be a developing homosexual orientation. The preceding formulation would suggest that efforts to promote heterosexual functioning should focus on those individuals who have not yet had extensive homosexual experiences. Obviously, much effort is needed by both the therapist and adolescent to clarify a sexual orientation that allows the individual to function comfortably. For many gender-disordered adolescents, support in adapting to a homosexual orientation, life-style and community living will be the most appropriate therapeutic direction. For those individuals who prefer to work toward a heterosexual orientation, the therapist should probably feel comfortable in discouraging homosexual experience unless it is clear that a comfortable level of heterosexual experience cannot be achieved.
Bradley’s framing of queer sexuality as a last resort, reserved for when “it is clear that a comfortable level of heterosexual experience cannot be achieved”, mirrors The Observer’s description of NHS England’s position that “social transition – treating a child as though they are of the opposite sex – should only be considered in cases where there is significant clinical distress or impairment in social functioning.”
The appeal to medical consequences of gay affirmation and gender affirmation
The Observer notes that gender-affirming puberty pausers are subject to “fears about potential long-term impacts for bone and brain development, fertility and sexual functioning; and concerns they make permanent gender dysphoria that would otherwise naturally resolve itself.” Yet anti-gay conversion groups, like ACPEDS in 2010, have similarly appealed to the supposed medical consequences of gay relationships and even gay self-identification, and warned of the dangers of “premature labeling” as gay:
Among adolescents who claim a “gay” identity, the health risks include higher rates of sexually transmitted infections, alcoholism, substance abuse, anxiety, depression and suicide. Encouragingly, the longer students delay self-labeling as “gay,” the less likely they are to experience these health risks. In fact, for each year an adolescent delays, the risk of suicide alone decreases by 20%. In light of these facts, it is clear that when well-intentioned but misinformed school personnel encourage students to “come out as gay” and be “affirmed,” there is a serious risk of erroneously labeling students (who may merely be experiencing transient sexual confusion and/or engaging in sexual experimentation). Premature labeling may then lead some adolescents into harmful homosexual behaviors that they otherwise would not pursue.
In a May 2017 letter, ACPEDS, CMDA, and the closely linked Catholic Medical Association (CMA) even claimed that “same-sex attractions” could be caused by “factors underlying the attractions” such as “peer dynamics, social media use and social contagion”, echoing arguments by anti-trans groups like SEGM and Genspect that gender dysphoria has a psychodynamic explanation and is spread through peer contagion and social media:
So called “conversion therapy bans” bar ethical talk therapy. Specifically, when minors present with unwanted same-sex attractions and/or gender dysphoria, therapists are prevented from exploring potential factors underlying the attractions or beliefs, including but not limited to, sexual abuse, family and peer dynamics, social media use and social contagion. Instead, therapists are required to engage solely in speech that affirms the child as lesbian, gay, bisexual or transgender. … The psychodynamic and social learning theories of homosexuality have never been disproven. There is good evidence that parental and social influences, including childhood trauma, can contribute to same sex attractions for some.
Members of ACPEDS, CMDA and CMA, including Quentin Van Meter (ACPEDS, CMA), Andre Van Mol (ACPEDS, CMDA), and Michelle Cretella (ACPEDS, CMA), have served in expert roles at the invitation of the DeSantis administration, helping the Florida Department of Health in developing expert reports to justify their desired restrictions on gender-affirming care.
The appeal to fluidity is undermined by the long-term stability of transgender identity
The Observer’s arguments for the exceptionalism of anti-trans therapy have been repeatedly marshalled in support of anti-gay conversion therapies, which are near-universally condemned as ineffective, a human rights violation, and an inherent affront to the dignity of LGBTQ people. They have been used by the same groups, and often the same individuals, to argue for some of the same “treatments” targeting both queer sexualities and transgender identities. These assertions of youthful gender fluidity also ignore published research indicating that transgender identity in youth is consistent and long-lasting, both before and after coming out as trans.
Olson et al. (2022) reported that in a sample of socially transitioned youth (average age 8.1 years at beginning of study), only 2.5% went on to identify as cisgender at an average followup of 5 years. Puckett et al. (2022), comparing identity milestones for four generations of trans people (Boomers, Gen X, Millennials, and Gen Z), found that all generations first felt different about their gender at average ages from 9-13 years old, and all of them took several years between first feeling different and recognizing their transgender identity. However, while Gen X first received gender-affirming treatment at an average of 35.6 years and Millennials at an average age of 23.1 years, Gen Z first received treatment at an average of 17.6 years old.
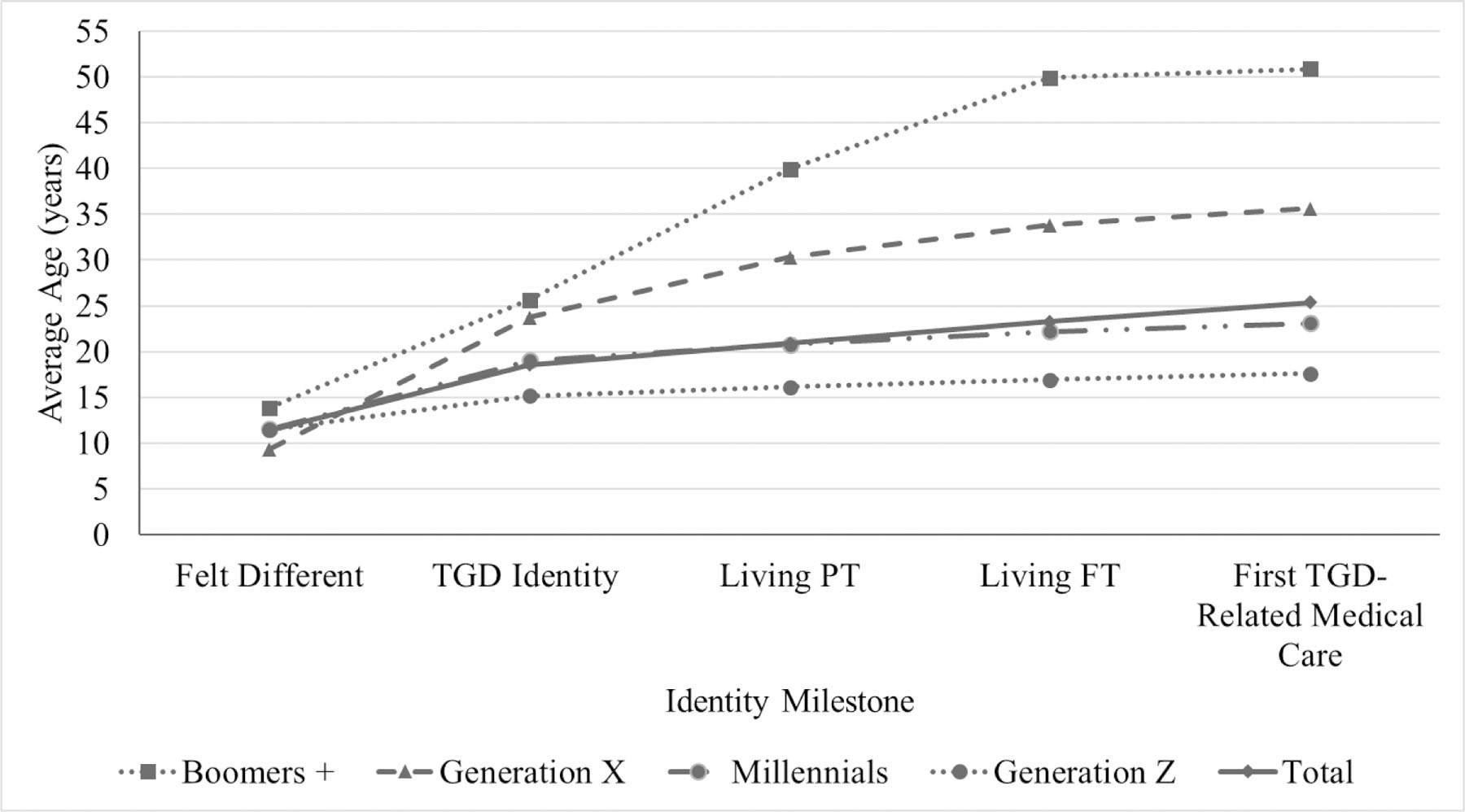
Puckett et al. (2022)
Because the timing of trans self-awareness has not changed, but the ages of coming out and transitioning have become lower in each generation, trans people who would have come out as adults in years past are instead now dismissed as flighty children with a transient fancy, simply because they were able to have access to trans terminology and concepts much earlier in their lives. Confirming this pattern of several years of gender self-awareness prior to first disclosure, a sample of 300 trans youth in Sorbara et al. (2020) found that they waited about 4.5 years to come out after first recognizing their gender incongruence.
Even non-affirming parents of trans youth have sometimes admitted in private anti-trans “support groups” that their children have consistently identified as trans for several years, and many of their children are now adults who continue to be trans. In a Genspect chat server in 2021, parent “R”, a mother in New York, recounts discovering this after reading her adult son’s childhood journals:
My own kid’s gender dysphoria seemed to be rapid-onset during her first year of college. But I did a terrible thing last week and read her journals from middle and high school (out of desperation to figure out what is going on) and found that she had been writing in her journal about gender ambivalence/dysphoria since she was about 12 or 13.
In the same server, parent “A” states that their child has identified as trans for five years:
Anyone have a therapist they can reccomend who isn’t affirmative ? Looking for help for my 19 year old daughter who is struggling this summer. Has identified as trans for 5 years.
And parent “S” hopes that her now 21-year-old trans daughter will stop being trans even after being out for six years:
This new of cohort of ROGD boys are embracing the transgender identity for many of the reasons the girls are. He started at 15 years old, just like Maddie. He is now 21, so I have a bit of hope he too may have an epiphany by mid twenties. That hope is what I hang on to to cope.
Parent “M” says her now-adult trans son has been out for three years:
Our neuro-typical daughter is 19 and has been doing the ftm thing for about three years.
Notably, while parent “C” addressed their 13-year-old’s trans identity by limiting their access to the internet, they acknowledge that this did nothing to make their now-adult child any less trans:
it may help you to know that we did Catch it quite quickly, took away all electronics, and even thoigh she had no real access to internet after that for years (age 13-15)- and then very limited after that until 18, it seemed to make no real diffidence.
Another parent, “G”, recognizes that these youth have been contemplating their gender identity for “months if not a couple of years”:
I think that the term rapid onset gender dysphoria (ROGD) is a bit unfortunate, because the kids think it dismisses their strongly held convictions as a fad. To them it does not seem rapid. They have been thinking about this for, ooh, months if not a couple of years, which is not rapid in their terms in their short lives.
For these parents, fluidity is clearly not a prominent feature of trans people’s gender identities – it is a matter of cis people’s wishful thinking. Behind these public invocations of fluidity, non-affirming parents are privately waiting years for their adult trans children to “desist”. The Observer does them no favors by encouraging this belief.
Involved groups
- Alliance for Therapeutic Choice and Scientific Integrity (ATCSI), formerly National Association for Research and Therapy of Homosexuality (NARTH)
- American College of Pediatricians (ACPEDS)
- Catholic Medical Association (CMA)
- Christian Concern
- Christian Medical & Dental Associations (CMDA)
- Core Issues Trust (CIT)
- International Federation for Therapeutic and Counselling Choice (IFTCC)
Key individuals
- Michelle Cretella (ACPEDS; ATCSI; CMA)
- Michael R. Davidson (CIT; IFTCC)
- Laura A. Haynes (IFTCC; ATCSI; ACPEDS consultant; CMA presenter)
- Christopher H. Rosik (ATCSI; IFTCC)
- Quentin Van Meter (ACPEDS; IFTCC; CMA)
- Andre Van Mol (ACPEDS; CMDA; IFTCC presenter)
Anti-gay and anti-trans conversion-related sources featuring fluidity arguments
- Neil Whitehead (of NARTH/ATCSI) and Briar Whitehead, “Can sexual orientation change?” (1999)
- NARTH, “Female Homosexual Development” (2008)
- CMA, “Homosexuality and Hope” (2008)
- ACPEDS, “Dear School Superintendent” (2010-03-31)
- ACPEDS, “What You Should Know About Sexual Orientation of Youth” (2010-04-01)
- Melinda Beck for the Wall Street Journal, “What To Say When Your Teenager Says She’s Gay” (2010-05-10)
- Affidavit of Michelle Cretella in Ferguson v. JONAH (2013-05-18)
- ACPEDS, “Empowering Parents of Gender Discordant and Same-Sex Attracted Children” (2014-06-13) (from DDoSecrets)
- ACPEDS, “Sexual Attractions and Youth” (2014-08-15) (from DDoSecrets)
- CIT and ATCSI, “Joint Statement in Support of UK Minister Morgan’s Call to End ‘Gay Cure’ Therapy” (2015-10-23) (cosigned by Michael Davidson, Christopher Rosik, Michelle Cretella)
- Christopher Rosik for ATCSI, “Sexual Attraction Fluidity Exploration in Therapy (SAFE-T): Creating a clearer impression of professional therapies that allow for change” (2016-05-27)
- Declaration of Michelle Cretella in Cochran v. City of Atlanta (ECF no. 57-12) (2016-08-25)
- Laura A. Haynes, “The American Psychological Association Says Born-That-Way-And-Can’t-Change Is Not True of Sexual Orientation and Gender Identity” (2016-09-27)
- “ACPeds, AAPS, CMDA and CMA Support Minors’ Right to Therapy” (2017-05-25)
- Declaration of Michelle Cretella in Sevier v. Fallin (ECF no. 1-43) (2017-10-24)
- ATCSI, “Guidelines for the Practice of Sexual Attraction Fluidity Exploration in Therapy” (2018-06-22)
- Michael Davidson for CIT, “A Response to the UK Government’s Proposed Ban on ‘Conversion Therapy’” (2018-09-13)
- Declaration of Michelle Cretella in Masterpiece Cakeshop v. Elenis (ECF no. 36-3) (2018-09-13)
- Declaration of Michelle Cretella in Guidry v. Elberson (ECF no. 15) (2018-09-19)
- Michael R. Davidson, Carys Moseley, and Christopher Rosik for IFTCC, “A Response to the UK Government’s Intended Ban on Therapeutic Choice” (2018-10-12)
- Laura A. Haynes for Public Discourse, “Are Religious Californians Really Harming the Mental Health of People Who Identify as LGBTQ?” (2019-09-16)
- IFTCC, “Postconference Statement 2019” (2019-11-17)
- Davidson, Rosik, Moseley, and Haynes for IFTCC, response to United Nations OHCHR call for input on so-called “conversion therapy” (2019-12-21)
- Child & Parental Rights Campaign, “School Resource Guide: Navigating the Transgender Landscape” (2020)
- IFTCC Conference (2020)
- IFTCC, “Serious Harmful Implications of Therapy Ban Bills” (2020)
- Laura A. Haynes for CMA, “Uncovering Treatable Causes of Same-Sex Attraction and Childhood Gender Dysphoria” (spring 2020)
- Declaration of Michelle Cretella in Cothran v. HHS (ECF no. 1-8) (2020-07-16)
- IFTCC letter to Canadian MPs (2020-11-18)
- Laura A. Haynes presentation for IFTCC, “Sexual Orientation and Gender Identity Change, May Have (Treatable) Psychological Causes” (2020-11-27)
- Genspect private support community for parents (2021-2022)
- Andre Van Mol for CMDA, “Evidence Opposing Therapy Bans” (2021-08-26)
- IFTCC submission to Norwegian MPs, “Oppose Conversion Practices Prohibition Legislation Bill” (2021-10-09)
- Laura A. Haynes at CMDA Student Life, “The Misnamed ‘Conversion Therapy’” (2021-11-06)
- Christian Concern, “Free to change – say ‘no’ to a ‘conversion therapy’ ban” (2021-12-03)
- IFTCC, “Extract from the submission to the UK Government’s Consultation on Conversion Therapy” (2022)
- Michael Davidson for The Critic, “Breaking faith” (2022-01-04)
- Declaration of Michelle Cretella in Pickup v. Biden (ECF no. 1-5) (2022-03-21)
- Michael R. Davidson, Laura A. Haynes, Steph James, and Peter May for IFTCC, “International Declaration on ‘Conversion Therapy’ and Therapeutic Choice” (2022-09-03)
- List of signatories (includes Core Issues Trust, Christian Concern, ATCSI, ACPEDS, CMDA, Liberty Counsel, Family Watch International, Society of Catholic Social Scientists, Islamic Leadership Institute of America, Fair Cop, Ruth Institute, Family First NZ, Andre Van Mol, Quentin Van Meter, Christopher Rosik, D. Paul Sullins, Mat Staver, Peter Sprigg, Sharon Slater)
- IFTCC, “Pastoral Protocol” (2023-05-20)
- IFTCC response to United Nations OHCHR “Call for inputs: Report on colonialism and sexual orientation and gender identity” (2023-05-26)
Further reading
- A New Era: Key Actors Behind Anti-Trans Conversion Therapy (Health Liberation Now!)
- TLRI Final Report 32: Sexual Orientation and Gender Identity Conversion Practices (Tasmanian Law Reform Institute, 2022)
- Interrogating Gender-Exploratory Therapy (Ashley, 2022)
- Transporting the Burden of Justification: The Unethicality of Transgender Conversion Practices (Ashley, 2022)
- The Parent Trap (Lux Magazine)
- How Therapists Are Trying to Convince Children That They’re Not Actually Trans (Slate)
- Leaked audio confirms Genspect director as anti-trans conversion therapist targeting youth (Health Liberation Now!)
- Unpacking ‘gender exploratory therapy,’ a new form of conversion therapy (Xtra Magazine)
- An Exploration of Conversion Therapy Practices in Ireland (Keogh et al., 2023)
- Conversion Therapy Online: The Players (Global Project Against Hate and Extremism)
More coverage from Gender Analysis
- Advisor to SEGM and Genspect taught Moms for Liberty to “play a dual game” and pretend to support parents who accept their trans kids
- Florida Medicaid agency paid thousands to Andre Van Mol to help ghostwrite their anti-trans policy
- Florida’s newest Boards of Medicine appointees wrote an anti-trans letter calling for gender “exploratory” therapy
- SEGM’s cofounder is an executive at the fifth-largest Catholic healthcare network in the US

If you’d like to help us with more investigations like this, you can support Gender Analysis on Ko-Fi or Patreon.

