
 Critics of transition treatments, opponents of transgender identity, and other anti-trans advocates have often claimed that trans people and our supporters have failed to address scientific findings that call into question the gender-affirmative approach. Ryan T. Anderson, a homophobic researcher at the conservative Heritage Foundation and author of the embarrassingly named “When Harry Became Sally”, provides a representative example:
Critics of transition treatments, opponents of transgender identity, and other anti-trans advocates have often claimed that trans people and our supporters have failed to address scientific findings that call into question the gender-affirmative approach. Ryan T. Anderson, a homophobic researcher at the conservative Heritage Foundation and author of the embarrassingly named “When Harry Became Sally”, provides a representative example:
…even as their own position shifts, the activists are absolutely closed off to contrary evidence. They call for the censure of honest researchers. They refuse to give any consideration to competing interests of privacy or safety. They reject alternative therapies that may be favored by parents or doctors.
All of this suggests a posture of defensiveness—that activists know their claims can’t stand up to scrutiny. The movement has to keep patching and shoring up its own beliefs, policing the faithful, coercing the heretics, and punishing apostates, because as soon as its furious efforts flag for a moment or someone successfully stands up to it, the whole charade is exposed. That’s what happens when your dogmas are so contrary to obvious, basic, everyday truths.
Contrary to this assertion that we’ve collectively refused to engage with anti-trans scientific claims, trans advocates have spent many years answering these arguments in detail – it is anti-trans critics who, ironically, have neglected to recognize the relevant research we’ve presented at length. Trans people have by no means shied away from listening to trans-critical scientific arguments, such as claims that transition is unnecessary, ineffective, or harmful; rather, we have repeatedly drawn attention to the most notorious purveyors of this scientific misinformation.
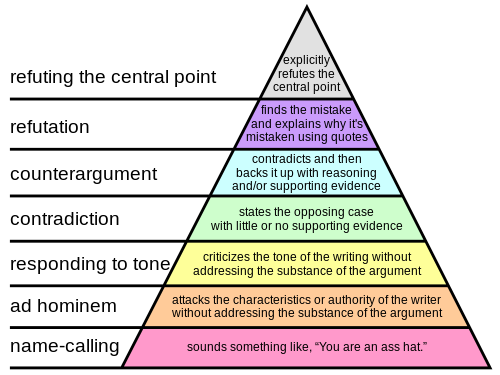
Anderson supposes trans advocates would be motivated to reject this science on the basis that it poses a real threat to our arguments. But there is no reason to believe such a threat is present. The weight of the relevant evidence is not split evenly between the positions of advocates and those of our critics. These critical claims are flawed in ways that strongly undermine their arguments, and we tend to address this at levels 5 (refutation) or 6 (explicitly refuting the central point) of the “pyramid of disagreement”:
Aim High
Nearly all anti-trans scientific claims are unsound, outright false, or plainly misleading, including those made by the foremost voices of public transphobia.
Paul McHugh. The Catholic former chief psychiatrist at Johns Hopkins University has become a prominent media figure, offering deceptive depictions of research on trans-affirming treatments. McHugh frequently references a methodologically flawed study (Meyer & Reter, 1979) to claim that trans surgeries do not improve health outcomes; the study declared trans people to be maladjusted if they had a same-sex partner or sought the recommended followup mental health care during and after transition. He later admitted his intention to discontinue trans healthcare at JHU from the very outset, even before the study in question had been conducted.
McHugh repeatedly misquotes a 2011 study of the Swedish trans population to claim that trans people who’ve transitioned have a greater likelihood of suicide; the study actually showed no elevation during the most recent decades, and the authors have explicitly rejected McHugh’s interpretation. He continues to publish his highly selective reviews of sexuality and gender research in The New Atlantis, a conservative religious journal.
Michelle Cretella. The president of the anti-trans American College of Pediatricians front group has falsely claimed there are “no cases in the scientific literature of gender-dysphoric children discontinuing blockers”; several such cases have been reported in the literature. Cretella publishes in the Journal of American Physicians and Surgeons, which has previously hosted AIDS denialism and an unretracted off-by-10 error that depicted undocumented immigrants as carriers of leprosy. Her articles have been published alongside anti-vaccination rhetoric and conspiracy theories about Andrew Breitbart being assassinated using cyanide. That is the level of credibility being brought to the table here.
Ken Zucker and Susan Bradley. The former heads of Toronto’s CAMH Child Gender Identity Clinic have recently made a name for themselves by suggesting that many children and adolescents with gender dysphoria may instead actually have autism. This notion is contradicted by the existing medical literature, which recognizes that autistic spectrum youth with gender dysphoria are genuine in their identities – these can be comorbid, and are clearly not mutually exclusive. Bradley additionally cites a Catholic blogger and claims that “trans activists” must be “unethically influencing autistic children to change genders”, her interpretation of a joint awareness campaign by the Autistic Self-Advocacy Network, National LGBTQ Task Force, and National Center for Transgender Equality.
I should also add that I spent nearly an hour debating Susan Bradley on these and other topics, as excerpted on I Am Jazz (4×03), after which a moderator told me I had won.
Detransition and regret. Claims that trans people experience high rates of regret, or are likely to choose to detransition, are commonly played up in anti-trans media. However, existing studies show that anywhere from 4% to 0% of trans people will regret having transitioned. Additionally, many of the supposed stories of regret cited by Federalist writers Walt Heyer and Stella Morabito have been twisted and misrepresented – these individuals often do not express regret, and several have chosen to re-transition.
“Rapid onset gender dysphoria”. This supposed phenomenon – the sudden appearance of gender dysphoria among teen trans boys – is actually the invention of members of three anti-trans websites, who filled out an anonymous online survey for a still-unpublished study on the subject. No clinical studies have been carried out to identify any features of this “new” population which distinguish them from other youth with gender dysphoria, nor is there any evidence that these youth began to experience dysphoria via some “social contagion” rather than revealing their already-present dysphoria.
Ray Blanchard and J. Michael Bailey, who would normally publish in sexology journals, have instead made one of those anti-trans sites their chosen venue for largely baseless speculation comparing this “condition” to social trends in “recovered memories” and diagnosis of dissociative identity disorder. Debra Soh further claims that youth with “rapid onset gender dysphoria” should instead be treated for “other mental-health conditions” such as borderline personality disorder, yet existing medical literature recognizes that trans people can genuinely experience gender dysphoria alongside personality disorders or other mental health conditions. Once again, comorbid conditions are not mutually exclusive.
Persistence and desistance in childhood gender dysphoria. Commentators including Debra Soh, James Cantor, and Ryan T. Anderson have asserted that anywhere between 60-95% of children with gender dysphoria will cease being dysphoric after starting puberty. These figures focus on probability when they should be focusing on probability distribution as more relevant to the outcomes of gender dysphoric youth. Because of the use of diagnostic criteria which could improperly group gender-nonconforming youth with gender dysphoric youth, this is not a homogeneous group. Youth whose gender dysphoria continues into adolescence typically display a stronger and more persistent cross-gender identity in childhood than those who desist in adolescence.
The figure of 60-95% of this heterogeneous group desisting at puberty wrongly suggests that an individual child can be assumed to have a 60-95% likelihood of desisting, when in reality their gender expression and intensity of dysphoric symptoms will place them into either a group of those likely to persist or a group of those likely to desist. Neglecting this bimodal distribution in favor of presenting overall probability alone is a willfully misleading portrayal of gender identity development in these youth.
Other questionable scientific notions, such as puberty blockers affecting vaginoplasty, treating dysphoria with antipsychotics, conflating dysphoria with body dysmorphia, and Ray Blanchard’s sexual etiology of trans women, have also been examined and dissected at length by trans advocates. What we’re being presented with here is not a pattern of strongly persuasive evidence consistently pointing towards a well-supported alternate model of transgender identity and care. It’s a pattern of poorly-informed arguments that fail to account for the current evidence and fall apart under the slightest scrutiny, a pattern of overt misrepresentations and omissions of facts, a pattern of conservative religious affiliation and avoiding medical journals that would hold their claims to a standard of evidence.
These anti-trans scientific claims begin to look less like a plausible competing model for explaining observed phenomena, and more like a kind of creation science of gender. These claims exist in their own parallel reality of made-to-order “alternative facts”, complete with faux authorities to promote faux explanations. It is not surprising that they do their best to avoid coming into contact with scientific findings contrary to their chosen beliefs. ■



{kind=link}
One Response to Most anti-transgender scientific claims are unsound