
Previously:
- CMA against Florida: Catholic Medical Association members Hruz, Van Meter, and Lappert have worked with Alliance Defending Freedom since 2017 to develop a group of anti-trans expert witnesses (September 2022)
- Catholic Medical Association members wrote a majority of Florida Medicaid’s anti-trans expert reports. Last year, CMA declared a faith-based commitment against approving of any transition care. (August 2022)
- Florida’s anti-trans expert Dr. Quentin L. Van Meter was discredited on trans youth care in court, believes trans people are “delusional”, and promotes anti-gay conversion therapy (July 2022)
- Dr. Stephen Levine and the Plot to Police America’s Gender (June 2022)
- Florida Department of Health Guidance Against Transgender Youth Healthcare Contains False Statements and Misrepresentations and Should Not Be Used by Anyone (April 2022)
On October 28, 2022, the Florida Board of Medicine and Florida Board of Osteopathic Medicine held a joint meeting to advance a politically-motivated ban on any medical transition treatment for youth under 18, including puberty blockers, HRT or surgeries, outside of yet-to-be-defined exceptions for “clinical trials”. This illegitimate process, featuring invited far-right experts with religious precommitments to transphobia and a DeSantis appointee on the Board working in secret with anti-trans groups SEGM and Genspect, is also the first time this medical transition care for youth has been banned at the state level by executive action rather than a legislative act.
Notably, the lineup of speakers for public comment started with nine detransitioners, and included six individuals currently working with the state of Florida to defend the state’s recent Medicaid trans care exclusion ban, with only six pro-trans voices allowed to speak against the proposed restrictions before public comment was closed. This process now advances to further rulemaking this coming Friday, November 4, at another joint meeting of the boards.
More coverage: Florida Board of Medicine Advances Ban on Transition-Related Care for Minors (Them.us)
In the interest of public discussion, my livetweeting of the proceedings as streamed by the Florida Channel is reproduced below in its raw entirety, with any known errors marked; other errors may remain. This is an initial update prior to an organized post summarizing today’s events, and an archived video from the Florida Channel is now available.
8:07 AM EDT
I’ll be taking notes on the proceedings in this thread. Previous thread on the contents of the meeting agenda and submitted public comments:
NEW: Florida Board of Medicine hearing on their sham rulemaking process to create an anti-trans standards of care is now RESCHEDULED to Friday, October 28 at 8:00 AM at the Hyatt Regency at Orlando International Airport: https://t.co/uSOWizZVYC
— Zinnia Jones | spookiest October ever (@ZJemptv) October 21, 2022
My previous notes on the involvement of the Catholic Medical Association and Alliance Defending Freedom in crafting the state of Florida’s trans care exclusions this year: genderanalysis.net
Patrick Hunter, appointed to the Board by DeSantis this summer, will be in attendance. Hunter has an undisclosed conflict of interest: He is a member of the CMA, which already made an absolute faith-based commitment against our standards of care in 2021 genderanalysis.net
Hunter also did not disclose his involvement in signing an anti-trans proposal to the American Academy of Pediatrics with SEGM’s director Julia Mason. Then Genspect blacked out his name, and Hunter promoted the letter without saying he was a signatory genderanalysis.net
Remarks by anti-trans expert Michael Biggs (8:17 AM)
Anti-trans activist Michael Biggs, a sociologist who is not a doctor, is reading off of something and delivering a fairly poor-quality livestream on “juvenile transsexuals”
Biggs attempts to claim any apparent improvement seen from use of puberty blockers in trans youth is due to a change in measures in a study “halfway through”; says 1 person contracting a lethal postsurgical infection common to hospital settings means there is a death rate over 1%
He’s leaning on that case report to say *puberty blockers* have a *death rate* over 1% (that case report has already been published), claiming youth on puberty blockers will have “no libido and no capacity for orgasm” (completely false)
The fatality noted by de Vries et al. (2014) was reported in greater detail by Negenborn et al. (2017) and describes a hospital-acquired infection with ESBL-producing E. coli, a type of antibiotic-resistant infection that is especially likely to be fatal (Melzer & Petersen, 2007). Because the risk of this kind of infection is not specific to gender-affirming surgery, any argument against gender-affirming surgery on this basis would require arguing against receiving surgery or going into hospitals for any purpose.
Biggs demanding that Florida only offer puberty blockers in a “randomized controlled trial” and “research protocol” as recently specified by the NHS England; Dr. David Diamond of the Board asks him what that research protocol is; Biggs says it isn’t available yet
Patrick Hunter predictably has that NHS England document on hand, explains NHS is still on the process of even crafting that “research program”
Remarks by pro-trans expert Dr. Kristin Dayton (8:29 AM)
Dr. Kristin Dayton of UF Health (pediatric endocrinologist, pro-trans expert) now videocalling in.
Patrick Hunter asking Dayton on data being kept on the patients; Dayton says they do not have an active registry of the patients; Hunter asking her to estimate which percent of youth at their clinic proceed to puberty blockers; Dayton estimates 20-30%
Hunter asks which percentage of those go on to receive HRT, Dayton says it is the vast majority; Hunter asks her to define the difference between “suicidality” and “completed suicide”
Hunter asking chair David Diamond to bring Biggs back to present his claims on suicidality; denied, maybe later
Hunter asking Dayton about “systematic reviews out of Sweden and out of England” referring to Socialstyrelsen and NICE evidence reviews, previously submitted and cited by the Florida Department of Health in April and in August
FLDOH describes the present guidance as “in line with the guidance, reviews, and recommendations” from Sweden and links to the March 2021 document “Good care of children and adolescents with gender dysphoria – National knowledge support” from the National Board of Health and Welfare, or Socialstyrelsen. But the Socialstyrelsen document repeatedly recommends comprehensive assessment for possible treatment of trans youth with puberty blockers and cross-sex hormones – it is not at all consistent with the FLDOH guidance against puberty blockers, hormone therapy, or even social gender transition for anyone under 18.
Remarks by pro-trans expert Dr. Aron Janssen (8:46 AM)
Dr. Aron Janssen, child and adolescent psychiatrist at Lurie Children’s Hospital, now videocalling in.
(The connection at various points here is terrible and keeps breaking up; having the experts videocall in was not a good idea)
Dr. David Diamond of the Board questioning Janssen, Diamond claims “colleagues in Europe” were “really the leaders” but now seem to make “a change” to “a more cautious and conservative approach”, claims the US is taking “a different approach”
Janssen asserts most US clinics follow Dutch model on this, and countries following that model such as the Netherlands and Belgium aren’t restricting such care now at all
David Diamond referring to interim findings from NHS Cass review
Diamond citing Cass review to say “how little we know” about use of puberty blockers because there’s “concern after concern mentioned”, cites July 19 letter from Cass to Dr. Stuart of NHS questioning “later-presenting young people, particularly biologic females”
(This is the standard ROGD/social contagion narrative, will get into the details on all this later but rapidonsetgenderdysphoria.com)
Remarks by anti-trans expert Dr. Riittakerttu Kaltiala (9:03 AM)
Next is Dr. Riittakerttu Kaltiala(-Heino), who has worked with Patrick Hunter (social contagion wolf story, ridiculous)
In articles from 2018/2020 by conversion therapist Robert Withers, Kaltiala claimed many trans kids had started telling her a story about pretending to be wolves. She attributed this to the same debunked ROGD “social contagion” Hunter cited at the Board. https://t.co/kaOhXOHhHM pic.twitter.com/gEgC8UWcvy
— Zinnia Jones | spookiest October ever (@ZJemptv) August 8, 2022
Kaltiala saying this care is centralized in Finland and is limited by law to “2 of the 5 universities” in the country
Kaltiala referencing COHERE Finland guidelines cited by Florida Dept of Health in April
Kaltiala claiming “up to 85%” of trans children who reach the early phases of puberty will not continue to be trans (desistance myth, but also corrects misrepresentations by Laidlaw et al. that you need to wait until *adulthood*)
Michael Laidlaw and friends still misunderstand the basics of affirming care for trans youth (May 2019)
Kaltiala says “exploratory therapy” and “exploratory intervention” is recommended, with any co-occurring mental health struggles having to be addressed first before referrals for gender identity assessments
(“Gender exploratory therapy” is a recently-developed euphemism now promoted for anti-trans, non-medical approaches typically involving disaffirming psychotherapy. Anti-trans therapists and other professionals and policymakers have organized under the label of “exploratory therapy” to describe attempts to delay trans youth and young adults from transitioning for as long as possible, under the assumption that gender dysphoria always has another cause that must be treated instead.)
Kaltiala stating these assessments last at least 6-12 months before puberty blockers. Explains why Kaltiala’s Finnish cohort cited by Florida was an average age of over 18 and did not show particularly good outcomes:
FLDOH cites Kaltiala et al. (2020) in its position that puberty blockers and hormone therapy should be unavailable to anyone under 18. However, Kaltiala et al. note that these youth were first diagnosed at a average age of 18.1 years (range 15.2-19.9) and all presented once the window for use of puberty blockers had passed, meaning all had experienced a gender-incongruent natal puberty. The authors cite this as a likely reason for the lack of change seen in the proportion showing good psychological functioning before and after treatment with hormone therapy.
(That clearly inadequate delaying approach is now being cited as a reason not to give puberty blockers to anyone when actually they obviously need to be given earlier)
Kaltiala past 10-minute mark and is being asked to wrap it up
Hunter now talking to Kaltiala and saying she said trans youth “could not have mental health issues” before transitioning, whereas Janssen and others cite studies showing improvement in mental health. Yeah, that is a good question and something she should have to explain
Kaltiala saying this is because “associated mental disorders impair the identity development”, referring to “severe psychiatric disorders”; Hunter is basically just letting her go overtime and continue monologuing
Kaltiala says “if the psychiatric problems seem more fundamental they have to be treated first”. These are mixed messages at best.
Hunter inviting her to continue monologuing again about her opinions on various evidence reviews, she says it is her opinion that “the evidence is lousy”; she criticizes the n=70 De Vries study for not having a control group (what control group, ideally??)
Kaltiala also asserts it is unclear which population the treatment group is representative of
Hunter asking Kaltiala why Sweden, Finland, NHS are making changes to availability of trans care, just a really open-ended continuation
Kaltiala asserting De Vries study and Dutch model were only applicable to childhood-onset dysphoria in AMABs (will get into this later because it is bullshit)
Lisa Littman cites Edwards-Leeper & Spack (2012) in her “rapid onset gender dysphoria” study – but did she read it? (December 2018)
SUBSET OF LATE-ADOLESCENT ONSET TRANSGENDER PATIENTS
Most adolescent patients who are seen in the GeMS clinic report histories of gender atypical behavior and severe gender dysphoria in childhood, and their parents recall this as well. These patients would likely have met the diagnostic criteria for gender identity disorder in childhood, had we evaluated them when younger. However, there is a subset of patients who have an atypical transgender identity development for one or more reasons. Most of these late-adolescent onset transgender patients indicate that they always felt different or knew that something was not right, but were unable to identify it until puberty. Oftentimes these individuals report that they initially thought that their confusion was related to sexual orientation because they were unaware that transgenderism existed. Others report that they were aware of feeling like the other gender, but either thought that there was nothing that could be done about it so they tried to ignore the feelings, or they feared how others would react if they expressed their gender dysphoria. Some of these patients recall attempting to inform a parent of their cross-gender identity but feeling quickly dismissed or rejected, making it difficult to bring up again. We find it common among these patients to report little or no early body dissatisfaction as it relates to their male or female anatomy. Sometimes these patients report having been unaware of the anatomical differences between males and females when younger, thus being oblivious to what they were missing. The awareness of one’s body not fitting with one’s affirmed gender seems to occur at puberty for many of these patients.
Kaltiala says puberty blockers and HRT should be “limited into the context of formal research studies”
Remarks by anti-trans expert Dr. Michael K. Laidlaw (9:23 AM)
Anti-trans expert Dr. Michael Laidlaw, pediatric endocrinologist, speaking now. Actually showed up in person, probably going to give the massive presentation I noted in the thread above (if he can whip through it in 10 minutes)
Says he has “a patient who is a detransitioner”. So that’s his experience
Laidlaw repeating the falsehood that “desistance” requires waiting until adulthood (this was addressed in 2019, he is misrepresenting things blatantly https://genderanalysis.net/2019/05/michael-laidlaw-and-friends-still-misunderstand-the-basics-of-affirming-care-for-trans-youth/)
In their letter to the editor, Laidlaw et al. stated that most “children” would “outgrow” their gender dysphoria “by adulthood”, inaccurately suggesting that adulthood rather than the onset of adolescence is the point at which gender dysphoria is observed to persist or desist. This is not the case: statistics about “desistance”, which are themselves often questionable and highly variable, are about whether or not childhood gender dysphoria persists beyond the onset of adolescence. Past that point, these dysphoric youth are unlikely to experience spontaneous remission of their dysphoria upon reaching adulthood – but Laidlaw et al.’s misrepresentation makes it seem as though this is the case. This is an attempt to provide a pretext for the continued denial of medically necessary care to gender-dysphoric adolescents, based on the false belief that it will simply go away within a few years and any affirming care would be unnecessary and inappropriate.
Astonishingly, it turns out that Michael Laidlaw, Michelle Cretella, and G. Kevin Donovan (2019) made a very similar error in an article published earlier this year in the American Journal of Bioethics.
(Note that G. Kevin Donovan is also a member of the Catholic Medical Association and contributed one of the five expert reports to Florida Medicaid in May; Michelle Cretella is a leader of the anti-LGBT “American College of Pediatricians” hoax expert group along with Florida Medicaid expert report writer Quentin Van Meter.)
Laidlaw talking about “basic biology”
His presentation is on page 136 of this 1.16 GB PDF https://ww10.doh.state.fl.us/pub/osteo/Osteo/10282022_RL_Publicbook.pdf
We’re back on this kind of metaphor

Laidlaw citing Dhejne 2011 study, extensively misused (https://transadvocate.com/fact-check-study-shows-transition-makes-trans-people-suicidal_n_15483.htm)
Laidlaw claims trans youth on puberty blockers have an “iatrogenic injury”, says there would be no further pubertal development “even when giving cross-sex hormones”
The source of this data is not provided. The Y axis is unlabeled

Laidlaw claiming taking estrogen causes trans women to have a 46-times increased risk of breast cancer; does not mention this is compared to cis men and is actually 3 times lower than cis women
Trans women and transfeminine people taking HRT are far less likely to develop prostate cancer (July 2020)
For instance, in 2019, the Telegraph breathlessly reported that the “risk of breast cancer rises 46 times for trans women after hormone therapy”. What this framing omitted is that the study found trans women had a 70% lower likelihood of developing breast cancer compared to cis women, that the “absolute risk of breast cancer in transgender people remains low”, and that “following breast cancer screening guidelines for cisgender people seems sufficient for transgender people using hormone treatment” (de Blok et al., 2019).
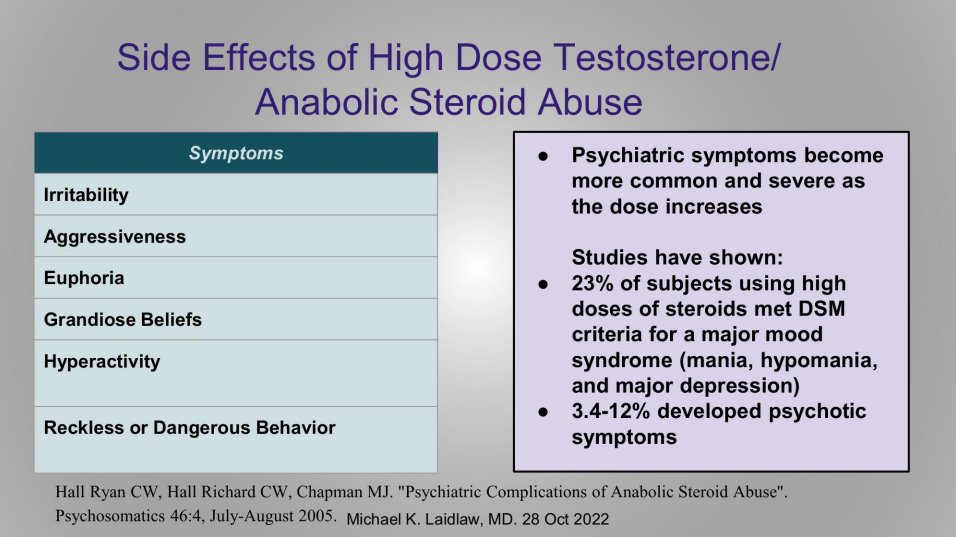
Laidlaw skipped over the part in his presentation where he cited a study on “anabolic steroid abuse” to criticize HRT
Laidlaw getting cut off for time, calls WPATH an “activist advocacy organization”
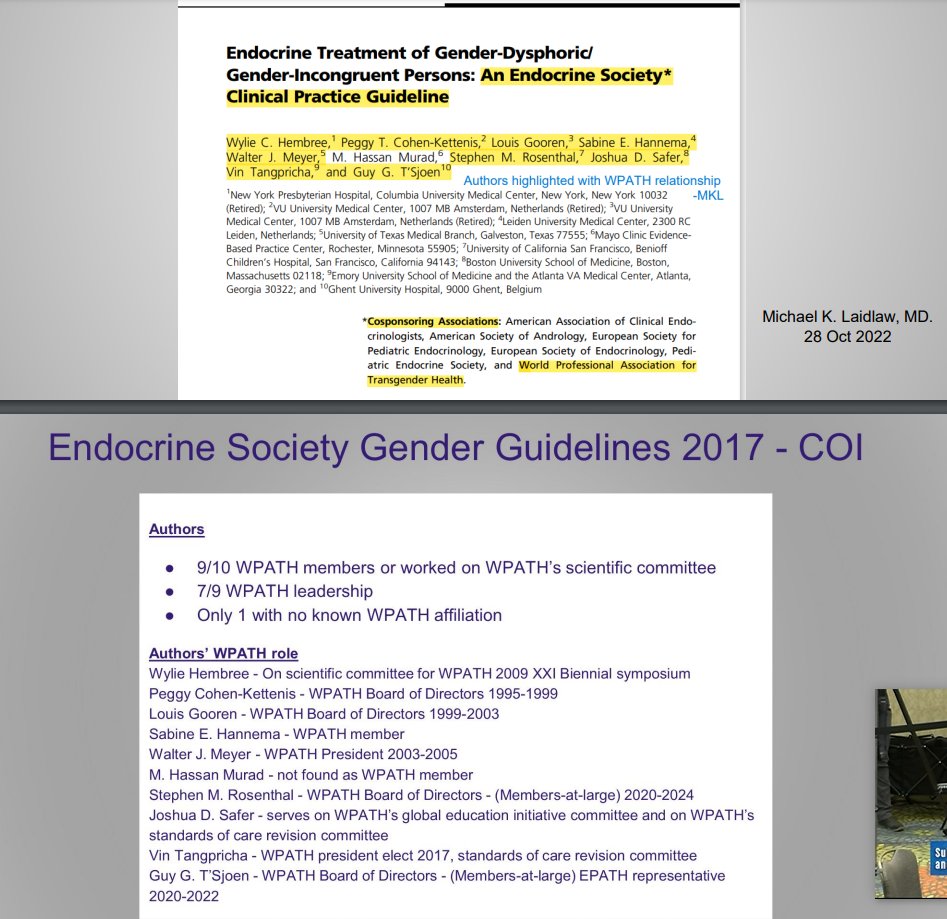
Laidlaw asserting WPATH and Endocrine Society conflicts of interest. We caring about conflicts of interest now?
Patrick Hunter saying there is a “50-90% desistance rate”, inviting Laidlaw to pontificate on this at length; Laidlaw saying lack of “desistance” after treatment is “not a fair comparison in any way”, likely arguing that social transition/puberty blockers cause persistence
Laidlaw asking “Are there any randomized controlled studies?” because those would be “high quality studies” but “don’t exist”
A board member, Dr. Tiffany Di Pietro (?) asking Laidlaw about Dhejne study participants and whether they were youth or adults. Laidlaw says it was adults, asserts on the basis of nothing that it “would be similar in children or worse”
Remarks by pro-trans expert Dr. Meredithe McNamara (9:39 AM)
Dr. Meredithe McNamara of Yale School of Medicine speaking now. Pro-trans expert, lead author on this critical report of Florida Medicaid’s trans exclusion https://medicine.yale.edu/lgbtqi/research/gender-affirming-care/florida%20report%20final%20july%208%202022%20accessible_443048_284_55174_v3.pdf
(My post on lower rates of breast cancer and prostate cancer in trans women: https://genderanalysis.net/2020/07/trans-women-and-transfeminine-people-taking-hrt-are-far-less-likely-to-develop-prostate-cancer/)
(“Social transition causes persistence” is an incorrect argument: https://genderanalysis.net/2022/06/dr-stephen-levine-and-the-plot-to-police-americas-gender-part-1/
“Puberty blockers cause persistence” appears similarly groundless: https://genderanalysis.net/2017/08/do-all-trans-youth-on-puberty-blockers-go-on-to-transition/)
Patrick Hunter hints at role of unnamed experts from McMaster University in Florida anti-trans process (9:52 AM)
Patrick Hunter says he’s making “more of a statement” and wants Meredithe McNamara to “comment”; says authors of the Florida June 2 literature review were trainees from McMaster University? We need to look into this
Of course it’s more of a statement, it’s completely unclear why this is relevant to anything
Patrick Hunter, ironically citing eminence over evidence, says McNamara can’t call Florida’s report authors “inexpert and not qualified” because they’re from McMaster University which apparently invented the phrase “evidence-based medicine”
(“Evidence versus eminence” is an anti-trans catchphrase used by the captured Florida health agencies since April 2022.)
Uh, imo that means they’re just people from a university who did a sucky job on that assignment
Can anyone identify who at McMaster University was involved in drafting anti-trans reports and literature reviews for the state of Florida this year?
(These trainees from McMaster University have since been identified as Romina Brignardello-Petersen and Wojtek Wiercioch of SEGM, who authored anti-trans Florida Medicaid Attachment C.)
Dr. David Diamond, chair of the board of medicine, asking McNamara about “obvious paradox” of Europe’s previous “more permissive” approach versus their “more conservative” approach now, compared to “more permissive” approach in US. McNamara says this isn’t what she’s seen.
Diamond interrupting her, saying NHS said puberty blockers would only be available under a “clinical trial”. McNamara points out that the word “trial” does not appear at any point in that document, there would be no randomization, and it would be observational
McNamara correctly points out this is intended to “roll out more prospective studies” (that is, enrolling patients *receiving gender-affirming care* and following up)
Dr. Diamond asking if at Yale, patients are referred for genital surgery at ages 16 or 17; McNamara says it is so rare she has never referred any patient for bottom surgery
Dr. Diamond asking the same about transmasc top surgery; McNamara says this is rare enough that she has never referred a patient for this; Diamond says he has seen patients referred at 16 for top surgery
A tense exchange between McNamara and board member Dr. Scot Ackerman (10:02 AM)
Patrick Hunter [Corrected: Scot Ackerman] asks “so why would you not refer a minor for surgical sex-affirming surgery?” if it is so beneficial. McNamara says this is because her patients hadn’t desired surgery and this is a shared decisionmaking process based on the patient’s desires.
Hunter [Corrected: Scot Ackerman] seems to have invented the word “phallusectomy”?
Outbreak of loud applause, cheers, various disruption
Board member Scot Ackerman also pointedly not understanding that these patients did not request surgery, McNamara explains it is a part of gender-affirming care for some individuals, Ackerman says “so you wouldn’t recommend it for anybody”. Blatantly disingenuous
McNamara seems to have gotten Ackerman to back down by explaining they do not appear to have a shared understanding of “recommendation”
I really hope that entire exchange was recorded
(This exchange begins at 2:16:44. McNamara refuses to reply to Ackerman’s request that she go on the record with an answer to an apparent false dilemma he was presenting; laughter and applause follow.)
Multiple board members conspicuously not understanding what it means to refer for an informed consent discussion with surgeons and the complexities of what this is rather than a strict yes/no “recommendation”
Board member Luz Marina Pages asking where kids are getting “affirmation” before referral for treatment. Dr. David Diamond asking whether it is in the “public interest of the great state of Florida” that 14 or 15 year olds should be able to obtain masculinizing top surgery
10-minute break (10:14 AM)
I think Dr. David Diamond’s phrasing reveals he does not consider trans youth and adults to be members of the public in Florida with a valid interest in state policy. In fact, they are the crucial stakeholders here, the ones whose bodies would be directly affected.
Trans people ARE the public. Trans people ARE the great state of Florida. So what the hell is wrong with you?
The remainder of the agenda according to the posted document:
- Discussion and Development of Rule Language
- Public Comments
- Closing Remarks and Administrative Matters
This whole process is a marathon and I have an outline ready for a more comprehensive post later today on the submissions to the meeting and the events today.
Genspect counterprogramming available here:
🧵 GENSPECT LIVE TWEETS from Florida Department of Health Board of Medicine meeting/workshop on RULE NO.64B8-9.019- “Practice Standards for the Treatment of Gender Dysphoria.”
— Genspect (@genspect) October 28, 2022
Details on the Finnish clinics mentioned by state anti-trans expert Dr. Riittakerttu Kaltiala. Includes harassing trans youth with questions about how often they look at their naked bodies and masturbate, criticizing their appearance and gender expression https://kehraaja-com.translate.goog/kuvaile-minulle-miten-masturboit-julkikuvan-takaa-paljastuu-transpolien-nuorten-synkka-tilanne/
Again, evidence produced by those Finnish clinics, showing low or no improvement for these youth – who were made to wait until an average age of 18 and were sexually harassed by that clinic! – is in turn cited by Florida Department of Health, Kaltiala’s friend Hunter, and so on
That title translates to: “”Tell me how you masturbate” – the position of trans youth in the health care system”
That Finnish model is the one that Kaltiala has helped craft, that Hunter, Biggs and others have expressed admiration of *as a model for trans youth care in Florida*
This is completely disgusting. Genspect are a real catch, too
Genspect document recommends that schools ban tucking. How big did Florida want the government – big enough to get into children’s pants? https://t.co/bYe4fBmpzZ pic.twitter.com/9nZNxKSSja
— Zinnia Jones | spookiest October ever (@ZJemptv) July 22, 2022
More on the anti-trans group Genspect and child safeguarding
Genspect, the “Genital Inspectors” who want schools to keep students from tucking (with an associate on Florida’s Board of Medicine), met with HHS civil rights division in April. A dad talked about bribing his trans kid with a puppy to show more cleavage https://t.co/FSC9FNr4fN pic.twitter.com/UBUfHf3YLO
— Zinnia Jones | spookiest October ever (@ZJemptv) August 2, 2022
DeSantis appointee Nicholas Romanello introduces a ban on under-18 medical transition care (10:31 PM)
Meeting resumes. Nicholas Romanello, an attorney, reminding the Board they are obligated to establish these practice standards. Seems to be saying they can’t decline to do so
Romanello talking about how for example medical marijuana requires an informed consent form. I suspect they may introduce the state forms from the previous meeting here (https://genderanalysis.net/2022/08/floridas-anti-trans-expert-dr-quentin-l-van-meter-was-discredited-on-trans-youth-care-in-court-believes-trans-people-are-delusional-and-promotes-anti-gay-conversion-ther/)
Romanello says he believes the risks of puberty blockers, HRT and surgery “outweigh the possible benefits and that there is a lack of consistent reliable scientific peer reviewed evidence concerning the efficacy and safety of such treatment”
Proposing a rule “to prohibit such therapies such as… G R H”
“… to treat gender affirming care or gender dysphoria for patients under the chronological care of 18”. Romanello makes it in the form of a motion, motion is seconded
Disgraceful moment
Scot Ackerman saying “there’s more to it than that that we need to get through regarding young Floridians who are in the process” and other youth receiving various related care
Scot Ackerman wanting to make sure these medications are still available for precocious puberty. Romanello saying motion talks specifically about “treatment of gender affirmation care or gender dysphoria” but “open to expanding that or contracting that … I would look to add”
Board member Zachariah P. Zachariah there will have to be a discussion by the committee, a period of public comment, and then vote
Patrick Hunter asserts psychotherapy should be the standard of care, questions competence of autistic trans people (10:38 AM)
Patrick Hunter wants the standard of care to include availability of psychotherapy for gender dysphoria and comorbid conditions, “the concern about the high rate of children with neurodevelopmental disorders” such as autism and ADHD
Read more: The anti-trans lie of “just autistic”; Playing both sides: Trans people, autism, and the two-faced claims of Ken Zucker and Susan Bradley; When it’s not “just autism”: ASD does not rule out gender dysphoria
“The diagnosis of ASD should not exclude an adolescent from also receiving a GD diagnosis and, when indicated, appropriate GD-related treatment. However, clinicians and parents sometimes dismiss GD as a trait of ASD (e.g., as an overfocused or unusual interest). Although in some cases GD symptoms appear to stem from ASD symptoms, many adolescents have persistent GD independent of their ASD.” (Strang et al., 2018)
“that this isn’t just a moratorium, but that the standard involves psychotherapy”
Board member Nicole Justice raises concern of unintended consequences on the population receiving this treatment (honestly it’s clearly entirely intended)
Someone please ask them what the strength of evidence is for whatever psychotherapy they propose
(Apologies if I mix up individuals here, I have face blindness issues)
Romanello proposes an “enhanced consent process” requiring at least four doctors of different specialties, comparing this to medical marijuana (10:41 AM)
Romanello: “My rule would be a prospective rule to take effect, I would look to board counsel to help on a prospective start date”
“so for those patients [currently in care] I would propose that we continue that care but that we, to insure the safety and to insure an educated and well-informed patient, that we enhance the consent process for those sorts of therapies”, compares this to MMJ dispensaries
“again very similar to what we did with marijuana”
“a multi-specialty type of consent” is what he is proposing – “a multidisciplinary approach”
“A multidisciplinary consent to include consent from pediatrics, endocrinology, psychology, and even I heard licensed clinical social workers”
“the second, similar to marijuana, would be highlighting and specifically documenting the patient’s attempt with alternative treatments for gender dysphoria or gender affirmation, counseling, the very beginning of the continuum before we get to puberty blockers and such”
“and finally a section where we would specifically require the identification of risks associated with the treatment”
“that they would have that list of risks presented to them at the time of treatment”
(These forms were previously proposed. They link to misinformation expert reports by Florida. 3 of 5 reports were by members of the Catholic Medical Association, precommitted to disapprove of this care. THIS IS STATE-MANDATED THEOCRATIC MISINFORMATION: https://genderanalysis.net/2022/08/floridas-anti-trans-expert-dr-quentin-l-van-meter-was-discredited-on-trans-youth-care-in-court-believes-trans-people-are-delusional-and-promotes-anti-gay-conversion-ther/)
Ackerman saying the joint committee (Board of Medicine/Board of Osteopathic Medicine) would meet next week to decide when this rule would go into effect
Next Friday, November 4
Board member Dr. Tiffany Di Pietro compares this process to screening out inauthentic letters for emotional support animals (10:49 AM)
Board member Tiffany Di Pietro saying children should have team of mental health counselor, pediatrician, pediatric endocrinologist, physician. Compares this to people who come to her with a letter saying they need an “emotional support animal”
Stop fucking dehumanizing trans people
Patrick Hunter proposes requirements to concentrate youth transition care in a small number of centers (10:50 AM)
Hunter: “I think mental health care should be part of the standard of care … we’ve heard that the research is very conflicted in this area … would a board rule have to include the option of research in this area?” raising possibility of IRB oversight, formal trials
Hunter saying puberty blockers etc should be brought into formal studies for “certainty of safety and ethical oversight”
Hunter: “it would have to be IRB-approved … I think I would prefer it being a center, like a university, a Florida medical school, I would be even more grateful if it involved international experts, Dr. Cass, Dr. Kaltiala in Finland”
Hunter says “I think we cannot be that specific at this point” because NHS hasn’t even formalized a protocol for research yet
Romanello: “it’s gonna have to be specific … you cannot just provide these general terms of an IRB-approved study in a university setting”
Romanello: “something that’s gonna have to be clear, understandable, defendable, and it’s gonna have to be written by next Friday”
Board member Dr. Sandra Schwemmer proposes a state registry of transgender children receiving medical care (10:55 AM)
Board member Sandra Schwemmer proposes families enter into a “registry, a Florida registry, that could monitor and give data back to the board” Boos from the crowd
Schwemmer: “I still think that registries are very helpful, so are the studies, but when you have a small participation in those studies…”
Schwemmer on registry: “I still think it opens an opportunity to be able to monitor this ongoing situation and therapies”
Schwemmer says it is for collecting data on those already in care. Ackerman says you can’t create a registry to “go around the rule”
Zachariah P. Zachariah: “Why would you register? What’s in it for you?”
Ackerman: “It’s anonymized”, talks about doing it for cancer
Zachariah: “That’s different”
Romanello: “we want to improve research in this area, for the betterment of all patients, we don’t want a rule then to inhibit or chill clinical research” Lie lie lie lie lie lie lie
Board member Dr. Scot Ackerman suggests state registry of trans youth could be “gamed” and research should only be conducted outside the state (11:00 AM)
Ed Tellechea: “So it’s a prohibition, except for under these circumstances … in a clear, enforceable manner”
Ackerman: “I think it can easily be gamed”
Hunter: “I probably would agree, but we need to learn more in this area”
Diamond talking about setting 18 as age for puberty blockers/HRT/surgery with “opportunity for exceptions to be made in the limited context of studies”
Ed Tellechea, chief assistant AG of the board of medicine: “The difficult thing is to define what a robust” process is and standards of care
Ackerman: “So people can do research, just not in Florida. I don’t think we need to make any comment about research. I think if there’s a rule there’s a rule, and the research can be done in… Yale”
Seems to be coming down to ill-defined exceptions, versus a blanket ban.
These people are some of the biggest dicks I have absolutely ever heard in my life
Diamond: “I would like to see this limited just to minors”
“Perhaps we have some comment now”
Public comments now, limited to 3 minutes each
Public comment period begins with nine detransitioners in a row, several of whom have testified for the state of Florida in the Medicaid exclusion case (11:05 AM)
Detransitioner Zoe Hawes appearing, Zoe Hawes is also part of the Dekker v Marstiller suit against the Florida Medicaid exclusion
(Declaration of Zoe Hawes in Dekker et al. v. Marstiller et al., 3 Oct 2022)
Hawes is complaining that her *church* affirmed her as trans
“I had a life-changing encounter with Jesus … I decided to detransition and accept my womanhood” Again, this person is working with the state of Florida to defend the Medicaid trans care exclusion
So Florida made sure she would be first up. Detransitioner Rachel Foster is next
Rachel Foster claiming intramuscular testosterone caused kidney failure
(Foster appears as a signatory to a letter on p. 820-825 of the public agenda.)
Detransitioner Chloe Cole next
(Cole entered a declaration in the redacted defendants’ response in opposition in Dekker et al. v. Marstiller et al., 3 Oct 2022. An article on MercatorNet about Cole is included on p. 839-841 of the public agenda.)
(Zinnia recommendation – we’ve found that it’s extremely good policy not to give detransitioners attention or engage with them due to constant massive attention-seeking pathology)
“My breasts were beautiful and now they have been incinerated for nothing, thank you modern medicine” as if to prove my point as I was typing that. Chloe Cole is 18
Detransitioner Camille (?) is next
(Camille Kiefel’s submission is on p. 1690 of the public agenda. Kiefel entered a declaration for the state of Florida in Dekker et al. v. Marstiller et al.)
“I can never fit a dress the same way again … who will love me?” continuously proving that I do know how to read people if they’re fucking overt enough about it
Detransitioner Shay (?)
(Others have identified Shay as an individual going by the name of “Shape Shifter” elsewhere. Shape Shifter’s submission appears on p. 830-834 of the public agenda.)
Alleges Christopher Salgado caused her to develop a rectovaginal fistula
Claims to have started detransitioning “a few months ago” and taking testosterone
Detransitioner Billy Burleigh, provided a submission in the agenda document linked above
(Burleigh’s submission is on p. 389-392 of the public agenda.)
Do you know how many trans people you’d have to scoop up before you get to *six detransitioners*? Proportional representation would easily have 100 happy trans people before 1 regretter. Instead we *lead with six detransitioners and counting* thanks to the DeSantis admin
This choice of lineup is directly intended to mislead the board about the basic situation of the vast majority of trans people receiving transition care. The DeSantis admin selected these people and made sure they would all be first in line before the board of medicine.
Next is detransitioner Catt Cattinson
(A new thread is begun at 11:23 AM.)
Catt Cattinson calls for no medical transition to be available to anyone *under age 25*
Next is detransitioner Helena Kirschner. Previously Kirschner blamed tumblr for her decision to transition, was cited by the Gospel Coalition, renounced gay sex and said she was “under the influence of gender ideology” when she had gay sex
This needs to be highlighted: despite all the accusations that we are “transing the gay away” or that cis gay kids are mistakenly transitioning, here’s The Gospel Coalition boosting someone who blames “gender” for her choice to have gay sex. Literally detransing the gay away. https://t.co/6TrqVZu6nu
— Zinnia Jones | spookiest October ever (@ZJemptv) October 26, 2022
Helena Kirschner, “By Any Other Name: The story of my transition and detransition.” (February 19, 2022)
That week was eventful, and I made a bunch of new trans friends. My roommate introduced me to his ex that he was still friends with, who at the time was also trans and eventually became my closest relationship for nearly four years (I will call her “Jamie”, and “she”, because that is how I know her now). She and I clicked immediately and would be inseparable for years, even long after any resemblance of a romantic relationship fizzled away. I consider myself heterosexual and would not date a trans man now, but at the time as a “gay trans man” under the influence of gender ideology, which tells you biological sex isn’t real, and experiencing surges of testosterone, I convinced myself I was attracted to this girl who looked like a boy at the time and had rapidly become my closest friend. Since in the back of my mind I knew she was a biological female, she didn’t intimidate me as much as actual men did.
Kirschner asks for rule “prioritizing exploratory psychotherapy”
(Kirschner’s submission is included on p. 786-815 of the public agenda.)
Not sure who this guy is but he’s thanking Dr. Michael Laidlaw – possibly this is the detransitioner Laidlaw talks about treating?
Talking about how electrolysis is “if you’ve never done that, it is painful”
I have. Stop being a drama queen
“I have two friends that have died in these procedures”, he says
“I was 50 when I transitioned, and it took me until 62 to figure it out” That’s what Florida and the DeSantis administration want for all of us. Fuck everything about that
Yaacov Sheinfeld, a parent who rejected his trans child, blames gender-affirming care for his child’s suicide (11:33 AM)
Next is Yaacov Sheinfeld, father of a trans child who committed suicide at 28, for the defense in Brandt v Rutledge and Dekker v Marstiller (Florida Medicaid exclusion) along with detransitioners
Brief in Brandt et al. v. Rutledge et al., 19 Nov 2021
Yaacov Sheinfeld was shocked when his wife told him that their 17-year-old daughter had announced she was transgender. Their daughter, S., had been in counseling for depression since she was 15 but never said anything about gender dysphoria.
Sheinfeld’s child was diagnosed and treated for depression before transitioning, but Sheinfeld attributes their suicide to testosterone without substantiating this as a cause
More on Sheinfeld later
Everyone calling time on Sheinfeld. Someone says she put her speaker card in SECOND and all these people were put before her
Sheinfeld, in his previous testimony, said that seeing his child’s body masculinize under testosterone made him want to commit suicide. But then he blamed trans people for emotionally blackmailing their parents with suicide threats
Declaration of Yaacov Sheinfeld in Dekker et al. v. Marstiller et al., 3 Oct 2022
13 . I witnessed distressing physical and emotional changes in S. The changes in her because of the testosterone were so distressing that I even considered suicide at one time.
…
20 . Florida’s Rule protects parents from being coerced into supporting these decisions through manipulation and threats like the one leveled at me that my daughter would commit suicide if she did not get the intervention she demanded.
Now calling Bob Flynn but multiple people have stood up and will not sit down. Yaacov Sheinfeld has to be escorted off
Six pro-trans speakers are called in total, interspersed with six anti-trans speakers (11:38 AM)
Dr. Mary Flynn, consulting psychologist, mother of trans child. “Everything we’ve heard before is nothing that I’ve ever heard in any support group, from any physician”
Blaise Treatise (?) expressing support for the rule and for state surgeon general Joseph Ladapo’s anti-trans reports and proposals, says “there is no care being provided, only child abuse”, “social media such as tiktok promotes gender dysphoria” Laughter from crowd
Calling trans women “patriarchal men dominating them, women” to quiet jeers
Talking about swimming and athletics, “womanhood is not a mental disorder suffered by men” Wow just gathering so much evidence today
Hope McClay (?) and her mother, pro-trans, has a trans child
Again, I hope there is a recording of this later so we can review it, these are just me summarizing as quickly as I can. @TheDaraKam @floridachannel?
“It would be psychologically damaging for her siblings, for our family” for her trans daughter to have to go through unwanted male puberty
Next is Dr. Edward Grass (?) general internal medicine and family practice, was on hospital ethics committee, against availability of any puberty blockers or cross-sex hormones, says LGBT people have “significant levels of mental illness that has not been satisfactorily addressed
Continuing to promote ROGD/social contagion/”only in adolescent AFABs” narrative (https://rapidonsetgenderdysphoria.com)
Saying NHS England “has reversed course in its transgender treatment advice”, calls trans youth “gender-confused”. Crowd calls time loudly, board asking crowd to be quiet
Next is Ada Lopez (?), pro-trans, mom of trans child
Next is Dr. Robert Roper (?) with case report of patient “C.G.” who claims to have suffered irreversible harm from transitioning
(C. G. entered a declaration for the state of Florida in Dekker et al. v. Marstiller et al.)
Says C.G. had autism, may need to look this person up in legal briefs in the relevant cases later
He said “angioplasty” when he meant vaginoplasty
Says this person started receiving blockers at a hospital in Providence, had vaginoplasty at 18, “my body is going to be a freak no matter what I do”
Next is Jude Spiegel, pro-trans, using time to read names of 17 trans youth who have committed suicide
Next is January Littlejohn, anti-trans, unaccepting parent of trans kid, had a submission in this 1.16 GB PDF https://ww10.doh.state.fl.us/pub/osteo/Osteo/10282022_RL_Publicbook.pdf
(Littlejohn’s submission is on p. 1608-1609.)
Talking about keeping child away from “internet influencers, limiting her internet use”
“had been encouraged by peers and influencers”
“I shudder to think what would have happened if we had affirmed her trans identity”, says they did “watchful waiting”, “after several years our daughter has desisted”
Says youth are “being encouraged through activism to dissassociate from their bodies”
Next is Jennifer Engles (?), licensed mental health counselor in Florida, pro-trans
Next is Bob Framingham, anti-trans (possibly linked to Julie Framingham from public submissions above?), says he’s been impacted by “watching my son transition”, “now he can’t lift 40 pounds”
(Robert and Julie Framingham’s submission is on p. 506-507 of the public agenda. Julie Framingham entered a declaration for the state of Florida in Dekker et al. v. Marstiller et al.)
Identifies their child as “Tyler”
Next is Dr. Kevin Astol (?) with University of South Florida, pro-trans, “the board does not know what is actually being practiced in medical care today”, criticizing Ackerman for saying only 49 other states can do research on this, makes Florida second-class in research
Calls Patty Sullivan (?) to speaker’s podium, says she will be last for day, met with jeers, Zachariah P. Zachariah offers them an email address to send in comments
The board is met with outrage at the closure of comments and the insulting offer of an email address (12:12 PM)
“THEIR BLOOD IS ON YOUR HANDS” chant erupts
Patty Sullivan is with Parental Rights Florida, says AMA and AAP are wrong, says Board of Medicine needs to make this law, someone in audience shouts SHAME! SHAME!
Sullivan interrupted with shout of BULLSHIT!
Sullivan citing Dhejne 2011 suicide misinformation again
State representative Anna V. Eskamani of Orlando asks to address the board on behalf of her constituents and is denied (12:17 PM)
Zachariah closes public comment for 5 minute break, a representative from Orlando (Anna Eskamani?) interrupts saying she represents her constituents
Room erupting in shouts from the crowd. LET THEM SPEAK! LET THEM SPEAK!
Audio to Florida Channel stream has been cut.
This is absolutely going about as badly as could be expected
People can be seen in the back of the audience gesturing animatedly.
Audio cuts in. “The governor gets you a seat on this sham board! Open secrets dot com, folks, look it up!” Talking about drafting rule now, related to informed consent form, “enhanced consent”.
Romanello continues advancing the proposed “enhanced informed consent” rule (12:32 PM)
Romanello citing Dayton and McNamara (pro-trans) to claim any consent should be “on a multi-practitioner basis” and “who specifically should be on that panel” – “pediatrics, psychiatry, endocrinology … support and mental health counseling”, suggesting an LCSW
Now recommending enhanced informed consent form with pediatrician, psychiatrist, pediatric endocrinologist, LCSW; questioning whether it should be a psychiatrist or a psychologist
Patrick Hunter: “any consent needs to recognize and share with the family the level of evidence and what the studies have shown”
Patrick Hunter equates youth social transition to committing to surgery and requiring the same capacity for informed consent (12:35 PM)
Hunter: “any informed consent needs to disclose the degree of evidence or lack thereof”, “informed consent is not a simple process”, “once you’re on the path of social transition, there is good evidence that transition maintains that persistence” saying it leads to surgery always
Saying 12 year olds would need to be able to consent to future surgery because it is implied, says multidisciplinary consent panel should include a surgeon
Dr. David Diamond saying he does not agree a surgeon should be involved, appreciates where it is coming from but logistics may be difficult
Diamond discussing “whether or not to proceed with the research exemption”, “in terms of language to help you” offers an exception that minors can be treated with GnRH/HRT as part of university-sponsored IRB-approved longitudinal study that the parents consent to
And that the study must be presented to the rules and legislative committee as a first step. Being told they may not have the authority to require the approval of such a process
Hunter saying that research should be required to follow everyone into adulthood per NHS. Stream is repeatedly cutting in and out.
Diamond asking how this works when someone reaches the age of majority, how they can mandate that participation could continue when they are not regulating the care of individuals 18 or older. Still cutting in and out.
Hunter says this would require “long term longitudinal followup”, Diamond is asking how they would require that
Diamond: “If you drop off, it’s a free country, you can’t do anything about that, there’s no way to mandate that”. Hunter agrees
Board member Dr. Sandra Schwemmer proposes requiring two psychological evaluations before medical transition for youth (12:45 PM)
Sandra Schwemmer who previously proposed a state registry of trans kids is now proposing “at least two psychological evaluations” or “two behavioral health evaluations”
Zachariah says he strongly believes “these minors should have psychological evaluations” rather than social workers or LCSWs
Zachariah: “My concern is a majority have significant psychological issues” and wants to see if this can be “resolved in some other fashion” (other than transitioning)
Schwemmer: “What I’m hearing is we’ve almost got a staged evaluation”, talking about consent again and therapy again at every stage
Diamond talking about kids currently receiving care: “but as a condition to continue, there must be a documentation of this more enhanced consent within a period of time”
Schwemmer talking about “the consent’s already there, but do we want to add the additional consent for the therapy, for the medication”
“Enhanced consent process” seems to be the term they are converging on for a highly restrictive proposal to concentrate provision of transition care in minors to a limited number of centers, possibly one, that can probably only bear a certain caseload, would be easily targeted
Romanello suggesting separate and progressive informed consent requirements for: puberty blockers; HRT; surgery
Hunter: “and I think everyone has a problem worldwide in this consent area, is there is so much that is unknown”, questioning whether those under 18 with mental health issues can understand this and therefore consent to this, says it is experimental because “so much is unknown”
Hunter: “but the ability to get informed consent is nearly impossible”
(So how are you going to collect that data??)
The board converges on a requirement of at least four specialists (12:54 PM)
Asking chief assistant AG of BoM Ed Tellechea what he needs today to draft this rule, Romanello says it would need to be panel of pediatric endocrinologist, pediatrician, psychologist and LCSW or something along those lines. Still going back and forth on specifics
Amy Derick of Board saying people already undergoing treatment should not need to extensively consent to this again, Diamond says “the rule just says you need to be aware of these complexities” but then proceeds to reiterate they do need the signoff from that whole panel again
Derick: “For the record, I’m not aware of how that’s different from what’s currently happening” in gender clinics
Hunter: “I think what the Dutch described” is that informed consent is not a form, it’s a long process of at least 6 months or longer than that
Hunter “Let me float this idea”
- that psychological care be the standard
- moratorium on any medical care under 18
- clinical trial would be only way to go forward under 18
Tiffany Di Pietro asks “who is responsible” for the care ultimately, someone says it would be the prescriber
Luz Marina Pages talking about who would run the clinical trials, Diamond saying it would need to be an IRB-approved clinical trial at a university-affiliated center, Tellechea says we can’t create trials through standards of practice rules, is beyond rulemaking authority
Board preparing to vote on this motion. Romanello saying this is not dealing with informed consent now, but down the line. Saying they’re doing the under-18 medical ban now unless with university-affiliated IRB-approved trial, rule is prospective.
Will define the rule “exclusively to minors with gender dysphoria”, not people who have reached the age of majority or with other conditions
“We have a hard stop on this meeting, it was noticed until 1 o’clock”. Calls from crowd to stop the voting
The board votes to advance the rulemaking process and prohibit medical care for trans minors (1:04 PM)
3 opposed. Calls from crowd
Crowd continues to shout. Motion passes, meeting is adjourned. Presumably this will continue at the board meeting next Friday, November 4: https://flboardofmedicine.gov/meeting-information/ https://ww10.doh.state.fl.us/pub/medicine/Agenda_Info/Public_Information/Agendas/2022/November/11042022_JointFB_Agenda.pdf.
Holiday Inn, Disney Springs @ 2:00p.m. ET, 1805 Hotel Plaza Boulevard, Lake Buena Vista, FL 32830
https://flboardofmedicine.gov/meeting-information/upcoming-meetings/.
To be clear, the motion passed to advance a ban on medical care for trans youth under 18, with details to come on any exceptions where this would be allowed in clinical trial settings. This rulemaking process will continue next Friday.
1:07 PM.


