
Here’s how to submit your comments on proposed Rule 64B8-9.019 (Florida Board of Medicine) and proposed Rule 64B15-14.014 (Florida Board of Osteopathic Medicine).
Previously:
- Tracking organized anti-trans submissions to the Florida Board of Medicine October 28 meeting, which passed a ban on medical transition for trans youth
- Florida Department of Health Guidance Against Transgender Youth Healthcare Contains False Statements and Misrepresentations and Should Not Be Used by Anyone
Short title: Gender Analysis FLBOM complaint 1
On November 14, the Florida Board of Medicine (BOM) and Florida Board of Osteopathic Medicine (BoOM, collectively the Boards) published their proposed rules to ban medical transition treatment for transgender minors, opening a 21-day comment period before these rules take effect on December 5. The BOM’s Rule 64B8-9.019 (“Standards of Practice for the Treatment of Gender Dysphoria in Minors”) is a blanket ban on puberty blockers, HRT or gender-affirming surgery for trans youth under 18, with exceptions for those currently receiving medical treatment:
(1) The following therapies and procedures performed for the treatment of gender dysphoria in minors are prohibited.
(a) Sex reassignment surgeries, or any other surgical procedures, that alter primary or secondary sexual characteristics.
(b) Puberty blocking, hormone, and hormone antagonist therapies.
(2) Minors being treated with puberty blocking, hormone, or hormone antagonist therapies prior to the effective date of this rule may continue with such therapies.
The Notice of Proposed Rule (26536889) states that a hearing can be requested by contacting BOM executive director Paul Vazquez:
IF REQUESTED WITHIN 21 DAYS OF THE DATE OF THIS NOTICE, A HEARING WILL BE SCHEDULED AND ANNOUNCED IN THE FAR.
THE PERSON TO BE CONTACTED REGARDING THE PROPOSED RULE IS: Paul Vazquez, J.D., Executive Director, Board of Medicine/MQA, 4052 Bald Cypress Way, Bin #C03, Tallahassee, Florida 32399-3253, Paul.Vazquez@flhealth.gov
Comments can also be submitted through a form on the Notice page. The Board of Osteopathic Medicine’s Rule 64B15-14.014 (“Standards of Practice for the Treatment of Gender Dysphoria in Minors”) is substantially the same ban, with a limited exception for use of puberty blockers and HRT in certain clinical trial settings, applying only to the small proportion of doctors who hold a D.O. degree:
(1) The following therapies and procedures performed for the treatment of gender dysphoria in minors are prohibited.
(a) Sex reassignment surgeries, or any other surgical procedures, that alter primary or secondary sexual characteristics.
(b) Puberty blocking, hormone, and hormone antagonist therapies.
(2) Nonsurgical treatments for the treatment of gender dysphoria in minors may continue to be performed under the auspices of Institutional Review Board (IRB) approved, investigator-initiated clinical trials conducted at any of the Florida medical schools set forth in Section 458.3145(1)(i), Florida Statutes. Such clinical trials must include long term longitudinal assessments of the patients’ physiologic and psychologic outcomes.
(3) Minors being treated with puberty blocking, hormone, or hormone antagonist therapies prior to the effective date of this rule may continue with such therapies.
Similarly, this Notice of Proposed Rule (26536986) states that a hearing can be requested by contacting BOM executive director Danielle Terrell:
IF REQUESTED WITHIN 21 DAYS OF THE DATE OF THIS NOTICE, A HEARING WILL BE SCHEDULED AND ANNOUNCED IN THE FAR.
THE PERSON TO BE CONTACTED REGARDING THE PROPOSED RULE IS: Danielle Terrell, Executive Director, Board of Osteopathic Medicine/MQA, 4052 Bald Cypress Way, Bin #C06, Tallahassee, Florida 32399-3256, or by email at Danielle.Terrell@flhealth.com.
The November 4 meeting notice (p. 2) specifies the materials required for any appeals of the Boards’ decisions:
If any person decides to appeal any decision made by the Board with respect to any matter considered at this meeting or hearing, he/she will need to ensure that a verbatim record of the proceeding is made, including the testimony and evidence from which the appeal is to be issued.
In our capacity as the organization Gender Analysis of Seminole County, Florida, we call for a hearing on undisclosed conflicts of interest, patterns of bias and additional improper actions by the Board of Medicine and Board of Osteopathic Medicine during the rulemaking processes of proposed Rules 64B8-9.019 and 64B15-14.014 F.A.C., including but not limited to:
- Disregard for evidence of any quality and the findings of clinicians and researchers with relevant expertise in care for trans youth.
- Heavy reliance on marginal opinions offered by small anti-trans advocacy groups, which do not constitute evidence, in formulating the proposed Rules, contrary to the Boards’ intended purpose as apolitical bodies.
- Egregious misuse and misinterpretation of published studies on trans health outcomes and gender affirmation, frequently misrepresenting these findings as showing something that they do not.
- Undisclosed prior commitments by a BOM member and state experts to reject any practice standards incorporating gender-affirming care, as part of their membership in the religious anti-trans advocacy organizations Catholic Medical Association (CMA).
- Undisclosed cooperation between the Department of Health (FLDOH) and the Boards to provide a lineup of anti-trans speakers who are concurrently serving as witnesses for the Florida Agency for Health Care Administration (AHCA) in the ongoing Medicaid exclusion case Dekker et al. v. Marstiller et al.
- The BOM’s deliberate misrepresentation of anti-trans detransitioners as far more numerous than they are, using this lineup of a small number of heavily reused individuals who have repeated their claims in several other states.
- Undisclosed coordination between a BOM member and the anti-trans groups Society for Evidence-Based Gender Medicine (SEGM) and Genspect, to promote poorly-defined and unsupported anti-trans models of “care” for trans youth.
- Permitting intrusive personal attacks against the bodies of transgender Floridians while cutting off a pro-trans speaker’s criticism of Governor DeSantis’ administration, on the grounds of civility and decorum.
Due to the pervasive nature of these biases and conflicts of interest and the Boards’ continued failure to address these urgent issues of public concern, we additionally call for an independent investigation into the origins and course of the anti-trans rulemaking efforts of the Boards, FLDOH, AHCA and any other relevant state agencies, including the Executive Office of the Governor. Our detailed outline of the Boards’ improper actions is provided below, with requested actions on these matters where appropriate.
Scope of issues: Involved parties, materials, and events
Florida Board of Medicine and Florida Board of Osteopathic Medicine
- The August 5 BOM meeting and submitted materials (public book PDF, 1873 pages, last modified Aug. 2).
- The October 28 joint Boards meeting (video) and submitted materials (public book PDFs version A [3336 pages, last modified Oct. 20], B [3336 pages, last modified Oct. 21, 3:52 PM], C [3331 pages, last modified Oct. 21, 6:39 PM], and D [3887 pages, last modified Oct. 26]).
- The November 4 joint Boards meeting (video and audio) and submitted materials (public book PDFs version X [3887 pages, last modified Oct. 27] and version Y [4944 pages, created Nov. 2 and last modified Nov. 3]).
- Statements and actions during these meetings and in relation to these meetings by the BOM and the Boards collectively as well as individual members Dr. David Diamond (BOM chair), Dr. Patrick K. Hunter, Dr. Hector Vila and Dr. Zachariah P. Zachariah.
- Statements during these meetings by the state’s anti-trans experts Michael Biggs and Dr. Michael K. Laidlaw.
- Public comment during these meetings by selected anti-trans speakers including but not limited to Zoe Hawes, Chloe Cole, Camille Kiefel, Yaacov Sheinfeld, Dr. Robert Roper, Bob Framingham, Erin Brewer, Julie Framingham, and Amy Atterberry, as well as undisclosed coordination involving this speaker lineup by the Florida Department of Health and Florida Agency for Health Care Administration.
Florida Department of Health and state surgeon general Joseph A. Ladapo
- FLDOH April 20, 2022 document “Treatment of Gender Dysphoria for Children and Adolescents” and April 20 document “Treatment of Gender Dysphoria for Children and Adolescents: Fact check” and cited literature, enclosed with state surgeon general Joseph A. Ladapo’s June 2 letter to the BOM (Aug. 5 public book pp. 1-5, Oct. 28 public book version D pp. 2258-2262, Nov. 4 public book version Y pp. 3315-3319).
- FLDOH July 28 “Petition to Initiate Rulemaking Setting the Standard of Care for Treatment of Gender Dysphoria” (Aug. 5 public book pp. 870-877).
- FLDOH July 28 “proposed forms” (Exhibits C and D), requiring all adults seeking hormonal or surgical transition care in Florida to wait 24 hours sign state-mandated “informed consent” forms referring to the AHCA GAPMS findings and commissioned expert reports at ahca.myflorida.com (Aug. 5 public book pp. 1112-1113).
- FLDOH’s role in providing an imbalanced lineup of anti-trans speakers to Boards at the October 28 meeting, which led with nine anti-trans detransitioners, some of whom have provided affidavits for the state of Florida’s defense in the ongoing Medicaid transition care exclusion case Dekker et al. v. Marstiller et al.; they did not disclose this related work at the Boards’ hearings.
- Joseph Ladapo’s role in reviewing the medical records of an uninvolved transgender adult at the behest of their anti-trans parent Amy Atterberry, without any clear basis for this complaint other than an objection to trans people receiving transition care altogether (Amy Atterberry letter, Oct. 28 public book version D pp. 1251-1252).
Florida Agency for Health Care Administration and associated experts
- The June 2 report “Florida Medicaid Generally Accepted Professional Medical Standards Determination on the Treatment of Gender Dysphoria” (included in Aug. 5 public book pp. 606-651, Oct. 28 public book version D pp. 2863-2908, Nov. 4 public book version Y pp. 3920-3965), attributed to Romina Brignardello-Petersen and Wojtek Wiercioch by BOM member Dr. Patrick K. Hunter at the October 28 meeting (see Appendix A, time index 2:03:15).
- May 16 report Attachment C by Brignardello-Petersen & Wiercioch (included in Aug. 5 public book pp. 656-727, Oct. 28 public book version D pp. 2913-2984, Nov. 4 public book version Y pp. 3970-4041)
- May 17 report Attachment D by James M. Cantor (included in Aug. 5 public book pp. 728-790, Oct. 28 public book version D pp. 2985-3047, Nov. 4 public book version Y pp. 4042-4104).
- May 17 report Attachment E by Dr. Quentin L. Van Meter (included in Aug. 5 public book pp. 799-812, Oct. 28 public book version D pp. 3056-3069, Nov. 4 public book version Y pp. 4113-4126).
- May 17 report Attachment F by Dr. Patrick W. Lappert (included in Aug. 5 public book pp. 813-828, Oct. 28 public book version D pp. 3070-3085, Nov. 4 public book version Y pp. 4127-4142).
- May 16 report Attachment G by G. Kevin Donovan (included in Aug. 5 public book pp. 829-838, Oct. 28 public book version D pp. 3086-3095, Nov. 4 public book version Y pp. 4143-4152).
- AHCA and secretary Simone Marstiller, in their capacity as defendants in the transition care exclusion case Dekker et al. v. Marstiller et al., which features affidavits for the state of Florida by several anti-trans speakers, or parties related to the anti-trans speakers, at the October 28 and November 4 meetings (Redacted defendants’ response in opposition, October 3, 2022).
Grounds for hearing and inquiry on the Florida Board of Medicine and Florida Board of Osteopathic Medicine 2022 anti-trans rulemaking efforts
1. Three of the five expert reports reviewed in AHCA’s June 2 GAPMS determination, the basis for FLDOH’s rulemaking petition to BOM, were by members of the Catholic Medical Association who hold a prior absolute commitment as of 2021 to oppose any standard of care permitting transition
AHCA expert report writers Quentin L. Van Meter, Patrick W. Lappert, and G. Kevin Donovan (Attachments E, F, and G, respectively) are members of the Catholic Medical Association, a small right-wing group of 2,500 members who do not represent mainstream views in medicine or medical ethics. Declaration of Quentin Van Meter in American College of Pediatricians et al. v. Becerra et al., November 9, 2021:
13. I am a member of the Catholic Medical Association.
Patrick Lappert, “Catholic Medical Association – Medical Student and Resident Boot Camp”, February 25, 2017:
A graduate of Uniformed Services University, Patrick Lappert, MD, has served as the president and surgeon of Madison, Alabama’s Lappert Plastic Surgery since 2003. An experienced plastic surgeon and physician, Patrick Lappert, MD, is a member of several industry organizations, including the Catholic Medical Association (CMA).
“CMA Members Federally Appointed to The Human Fetal Tissue Research Ethics Advisory Board of National Institutes of Health”, Catholic Medical Association, August 10, 2020:
Doctors Greg Burke (Co-Chair of CMA’s Ethics Committee), Ashely Fernandes, Kevin Donovan and Father Tadeusz Pacholczyk, Ph.D. will work with other appointed members to advise the administration on the ethics of federally funded research which includes tissues from the bodies of babies who were aborted.
CMA has argued in legal actions that its members have “medical and ethical” conscience objections against agreeing to any transition treatment as part of a standard of care, based on their faith beliefs as adherents to this interpretation of Catholicism. Declaration of Mario Dickerson, executive director of CMA, in American College of Pediatricians v. Becerra, November 4, 2021 (see Appendix C for additional excerpts):
2. I serve as the Executive Director of the Catholic Medical Association (“CMA”). Given my involvement in CMA, I am familiar with the organization’s history, the issues confronting it, and the views of the organization and its members concerning various emerging issues, including the gender identify mandate at issue in this litigation.
3. CMA is the largest association of Catholic individuals in healthcare. CMA is a national, physician-led community that includes about 2500 physicians and health providers nationwide. […]
9. CMA’s mission is to inform, organize, and inspire its members, in steadfast fidelity to the teachings of the Catholic Church, to uphold the principles of the Catholic faith in the science and practice of medicine. […]
50. In accord with these scientific and religious understandings, CMA and its members believe that healthcare that provides gender-transition procedures and interventions is neither healthful nor caring; it is experimental and dangerous. […]
53. CMA thus opposes pubertal suppression of minors, as well as hormone administration or other surgical interventions for purposes of “choosing” a gender or sex, and it objects to engaging in speech affirming these gender interventions.
54. CMA has adopted an official resolution stating, “the Catholic Medical Association does not support the use of any hormones, hormone blocking agents or surgery in all human persons for the treatment of Gender Dysphoria.”
55. CMA has adopted an official resolution stating, “Catholic Medical Association and its members reject all policies that condition children to accept as normal a life of chemical and surgical impersonation of the opposite sex” as well as “the use of puberty blocking hormones and cross-sex hormones.” […]
Dickerson specifically notes CMA members’ beliefs and conscience prevent them from approving of gender-affirming medical treatment within a standards of care process:
69. The gender identity mandate requires CMA members to engage in various practices to which our members objection on medical and ethical grounds, including the following: […]
m. Saying in their professional opinions that these gender intervention procedures are the standard of care, are safe, are beneficial, are not experimental, or should otherwise be recommended; […]
For ease of reference, the items in this list will be referred to as the “objectionable practices.”
70. The objectionable practices violate the teachings of the Church, and our organization’s members cannot carry them out in good conscience. […]
130. Our members’ sincerely held religious beliefs prohibit them providing, offering, facilitating, or referring for gender transition interventions and also from engaging in or facilitating the objectionable practices.
The conflict arising in the context of the Boards’ rulemaking process is clear: Of AHCA’s five expert reports included in the June 2 report and used as the basis for FLDOH’s rulemaking petition to BOM, three of these – a majority – were authored by individuals who would not be able to issue any finding in favor of gender-affirming care under any condition. If, hypothetically, it were shown that the broad field of gender-affirming treatment has only highly positive outcomes and beneficial effects with no drawbacks whatsoever, these three authors would not be able to recognize this in the course of writing their reports on the evidence in this field. The reason they would not be able to recognize this is because of their preexisting commitment with an external private organization that they will never say “in their professional opinions that these gender intervention procedures are the standard of care, are safe, are beneficial, are not experimental, or should otherwise be recommended”.
This is a conflict of interest and would disqualify them from participating in any objective evaluation of evidence according to its intended purpose. Van Meter, Lappert, and Donovan did not disclose this conflict of interest in their reports to AHCA, nor did they decline to participate in this process on the basis of that conflict of interest. Romina Brignardello-Petersen and Wojtek Wiercioch, in their June 2 GAPMS determination report incorporating the five commissioned expert reports, did not note that this conflict of interest was present in a majority of the commissioned expert reports comprising their review. Brignardello-Petersen and Wiercioch note, twice, their heavy reliance on the five AHCA reports:
The determination process requires that “the Deputy Secretary for Medicaid will make the final determination as to whether the health service is consistent with GAPMS and not experimental or investigational” (Rule 59G-1.035, F.A.C.). In making that determination, Rule 59G-1.035, F.A.C., identifies several factors for consideration. Among other things, the rule contemplates the consideration of “recommendations or assessments by clinical or technical experts on the subject or field” (Rule 59G1.035(4)(f), F.A.C.). Accordingly, this report attaches five assessments from subject-matter experts:
Attachment C: Romina Brignardello-Petersen, DDS, MSc, PhD and Wojtek Wiercioch, MSc, PhD: Effects of Gender Affirming Therapies in People with Gender Dysphoria: Evaluation of the Best Available Evidence. 16 May 2022.
Attachment D: James Cantor, PhD: Science of Gender Dysphoria and Transsexualism. 17 May 2022.
Attachment E: Quentin Van Meter, MD: Concerns about Affirmation of an Incongruent Gender in a Child or Adolescent. 17 May 2022.
Attachment F: Patrick Lappert, MD: Surgical Procedures and Gender Dysphoria. 17 May 2022.
Attachment G: G. Kevin Donovan, MD: Medical Experimentation without Informed Consent: An Ethicist’s View of Transgender Treatment for Children. 16 May 2022. […]
Five clinical and technical expert assessments attached to this report recommend against the use of such interventions to treat what is categorized as a mental health disorder (See attachments):
Health Care Research: Brignardello-Petersen and Wiercioch performed a systematic review that graded a multitude of studies. They conclude 3 that evidence supporting sex reassignment treatments is low or very low quality.
Clinical Psychology: Cantor provided a review of literature on all aspects of the subject, covering therapies, lack of research on suicidality, practice guidelines, and Western European coverage requirements.
Plastic Surgery: Lappert provided an evaluation explaining how surgical interventions are cosmetic with little to no supporting evidence to improve mental health, particularly those altering the chest.
Pediatric Endocrinology: Van Meter explains how children and adolescent brains are in continuous phases of development and how puberty suppression and cross-sex hormones can potentially affect appropriate neural maturation.
Bioethics: Donovan provides additional insight on the bioethics of administering these treatments, asserting that children and adolescents cannot provide truly informed consent.
In the June 2 GAPMS determination report, Brignardello-Petersen and Wiercioch also did not describe how their review would account for biases such as the majority of reviewed reports originating from authors who were certain to provide the same negative finding in all possible circumstances. FLDOH additionally failed to recognize or disclose legal risks to the state of Florida inherent in requiring transgender adults to sign forms affirming the accuracy of these religiously-motivated anti-trans AHCA reports (Exhibits C and D), a requirement that could have opened the state to costly legal action on the grounds of possible violations of the Free Exercise Clause and the Establishment Clause of the First Amendment. CMA’s suit American College of Pediatricians et al. v. Becerra et al. also relies heavily on arguments involving the protection of their members’ consciences in the context of legal requirements that may conflict with this, indicating that CMA members are aware of the potentially serious burdens of such requirements; see Appendix C paras. 23, 69-70, 130, 138.
The BOM should not have accepted the GAPMS report’s findings, and should not have accepted FLDOH’s petition for rulemaking on the basis of this report. Additionally, an inquiry is necessary into how AHCA or other state agencies located and selected these three CMA members to work in this area, given that this information about their preexisting commitment specific to this field was publicly available prior to 2022.
Further issues with the five AHCA reports collectively and individually are detailed by the Yale School of Medicine (“Public comments on Florida proposed rule denying Medicaid coverage for gender-affirming medical care”, July 8, 2022), including:
- Van Meter’s disqualification as an expert in youth gender dysphoria in a divorce case in Texas in 2020, and his undisclosed substantial reuse of a prior declaration in Adams v. School Board of St. Johns County (2017) as Attachment E for the AHCA.
- Lappert’s disqualification as an expert on gender dysphoria treatment in Kadel v. Folwell (2022), and his undisclosed previous work with the anti-trans Alliance Defending Freedom, which has worked to cultivate a stable of anti-trans expert witnesses (Deposition of Paul W. Hruz in Kadel v. Folwell, September 29, 2021; deposition of Patrick W. Lappert in Kadel v. Folwell, September 30, 2021).
- Cantor’s undisclosed reuse of his work with the ADF in B.P.J. v. West Virginia State Board of Education (2022) as Attachment D, and the finding in Eknes-Tucker v. Marshall (2022) that Cantor does not have experience in treating gender-dysphoric youth.
2. BOM member Dr. Patrick K. Hunter is a member of CMA, holds the same prior commitment against any standard of care permitting transition, and did not disclose this or recuse himself
Dr. Patrick K. Hunter was appointed by Governor Ron DeSantis to the Florida Board of Medicine on June 17, 2022 (“Governor Ron DeSantis Appoints Four to the Board of Medicine”, June 17, 2022). Hunter was also confirmed to be a member of the Catholic Medical Association in July 2019. Diocese of Orlando, “CMA students make a difference in NFP education and more”, July 25, 2019:
The Catholic Medical Association’s student chapter at UCF began with three medical students just three years ago. Kaitlyn Hite, Jais Emmanuel and Michael Mankbadi would gather to support each other in the faith. After participating in Mass at Nemours Children Hospital, a mutual friend connected them to the Catholic Medical Association Orlando Guild. Enter Dr. Peter Morrow, who was president that year. The introduction was a God moment. Morrow and friend, Dr. Patrick Hunter, had both been praying for the opportunity to establish a student guild at the university. In fact, the entire CMA Orlando guild was praying.
UCF College of Medicine, “Student Organizations & Student Events”:
Catholic Medical Association (CMA)
Faculty Advisor: Drs. Colleen Moran-Bano & Patrick Hunter
As with AHCA reports contributed by Van Meter, Lappert, and Donovan, Hunter’s CMA membership presents a conflict of interest in the context of his actions and statements as a Board member on standards of care for gender dysphoria. The Catholic Medical Association has specified precisely which treatments their members cannot support as part of a standard of care for transition treatment, including puberty blockers as well as HRT and gender-affirming surgery at any age. Again, if all available evidence were in favor of gender-affirming care, Hunter would not be able to recognize this because of his preexisting commitment to CMA not to accept these treatments as part of a standard of care.
This conflict of interest renders Hunter unable to evaluate the evidence and policymaking considerations at hand in a fair and objective manner, and should disqualify him from participating in any BOM proceedings on this subject. Instead, Hunter failed to disclose this conflict of interest, and failed to recuse himself from these proceedings. His actions as a BOM member have been in accordance with what is required him as a CMA member: Voting to advance bans on this care for trans youth at the August 5, October 28, and November 4 meetings, and specifically arguing at the November 4 meeting for a total ban without even an exemption for clinical trials, including entering a 10-minute statement into the record against gender-affirming care (see Appendix B, 23:56-33:52).
Hunter, as well as other BOM and BoOM members, AHCA and FLDOH staff, and their associated commissioned experts, should be required to disclose any membership in organizations such as CMA (and other groups in its umbrella organization Alliance for Hippocratic Medicine/AHM) which maintain a commitment against any positive evaluation of gender-affirming care. Members of these organizations should be required to recuse themselves from any proceedings on this issue.
3. BOM member Dr. Patrick K. Hunter failed to disclose his association and history of working with the anti-trans group SEGM and related group Genspect
Before being appointed to the BOM, Dr. Patrick Hunter cosigned Resolution #27 against gender-affirming care to the American Academy of Pediatrics on March 31, 2022 with director Julia W. Mason of SEGM and three others. Their resolution asserts that there has been a “near unified movement away from hormonal and surgical interventions as first line treatment in multiple countries”. A copy of this resolution with these names concealed was posted by Genspect (“An Open Letter to the American Academy of Pediatrics”, July 18, 2022), an organization documented by the Trans Safety Network and Health Liberation Now! as sharing a number of key leaders and advisors with SEGM (“SEGM uncovered: large anonymous payments funding dodgy science”, August 16, 2021; “A New Era: Key Actors Behind Anti-Trans Conversion Therapy”, June 1, 2022). The names of these signatories, including Hunter, were revealed on July 21, 2022 by Gender Analysis.

Hunter also retweeted Genspect’s open letter on his Twitter account without disclosing that he had signed the AAP resolution, while SEGM director Mason later argued on Twitter that the concealed signatories should not have been named (Tweet by @JuliaMasonMD1, July 21, 2022).
Hunter was present at an April 25, 2022 meeting requested by SEGM with the US Department of Health and Human Services Office of Civil Rights on “Nondiscrimination in Health Programs and Activities”, with fellow Resolution #27 signatories Julia W. Mason, Paula Brinkley, and Sarah B. Palmer. Notably, while the affiliations of Brinkley and Palmer were listed as “SELF”, Hunter’s affiliation was listed as “Society for Evidence-based Gender Medicine”. Hunter did not disclose his prior or current relevant work with SEGM or Genspect at any point during the Boards’ proceedings. However, he did rely heavily on their materials submitted to the Boards when calling for SEGM’s own proposed “community standard of care” for trans youth.
4. BOM member Dr. Patrick K. Hunter called for an undefined anti-trans “community standard of care” excluding affirmation and transition, a novel term first used in this context by the anti-trans group SEGM and not appearing elsewhere
At the November 4 meeting (see Appendix B, 24:09), BOM member Dr. Patrick Hunter seconded a motion to strike the clinical trial exemption from proposed Rule 64B8-9.019, and entered a statement into the record drawing heavily from SEGM’s October 27 submission to the Boards (public book version Y, pp. 33-45). Passages from SEGM’s Oct. 27 letter and Hunter’s highly similar remarks are compared below:
SEGM, ¶ 14. The “gender-affirming” model of care is relatively new and was scaled into practice without rigorous clinical research. Selected outcomes associated with using the so-called “Dutch protocol” to medically transition minors were published in 2014 in a case series of 55 patients. Many of the authors associated with the development of the Dutch protocol for medical transition of minors also authored The Endocrine Society guidelines for hormone administration to minors in 2009; these guidelines were updated in 2017, lowering the age of eligibly for medical interventions.
[24:09] DR. PATRICK HUNTER: “I want to read this into the record. Dutch researchers pioneered youth transition for gender dysphoria. They published several papers culminating in a 2014 paper that described the outcome for 55 youths they transitioned. The Dutch protocol is now what we call affirmative care: puberty blockers, cross-sex hormones, and breast and genital surgeries. The Dutch protocol was deemed a success because the youth continued to function well after surgery. This affirmative model of care has spread wildly in the last eight years.”
¶ 18. The practice of gender transition of minors rests largely on the results of one key study, which gave rise to the practice of pediatric gender transition worldwide. In 2014, Dutch clinicians reported on a carefully selected group of 55 youth who underwent gender transition. At follow-up 1.5 years post-surgery, the young adults (average age of 21) retained good psychological function. However, a comparison of pre- and post- transition improvements in psychological function found improvement was modest at best.
[24:56] HUNTER: “The Dutch protocol is the foundation youth transition was built on. It is flawed, it is based on weak evidence. These are some of the problems with the Dutch study. Many concerns have been raised about its methodology. It was a case series, a small cohort of 55 teenagers. There was no control group.”
¶ 19. The long-term outcomes of the cohort of the 55 young patients, beyond 1.5 years post-transition, have not been published.
¶ 20. The 2014 “Dutch study” revealed a significant risk of harm of the gender-affirming hormones and surgery pathway. One patient died due to surgical complications. Three of the original 70 cases experienced new onset diabetes or clinically severe obesity. Several others refused to participate or did not return their questionnaires, adding to the uncertainty about their outcomes.
[25:24] HUNTER: “The follow-up period was only 18 months. This short period should be of concern. And most importantly, there has been no long-term data reported on these 55. The Dutch have been asked for their long-term data. In a June New York Times article, Dr. de Vries, the lead author, said the Dutch has [sic] lost contact with 50% of their early cohort. Dr. de Vries was interviewed on an American podcast in January. She made it clear that their patients’ lives are much more complicated than the original study’s outcome suggests.”
¶ 21. The Dutch researchers were acutely aware of the risk of psychological harm from wrongly transitioning a young person whose identity is still undergoing development. Consequently, they developed strict inclusion criteria for youth gender transition.
[26:15] HUNTER: “The Dutch, to their credit, were concerned about false transitions – transitions that would later be regretted. False transitions would be the worst possible outcome. Today we call that regret and detransition. The Dutch had inclusion and exclusion criteria hoping to limit false transitions.”
¶ 24. 3. Severe gender dysphoria from early childhood that worsens in adolescence. Only children with severe early-onset gender dysphoria were considered for medical gender transition. Those whose gender dysphoria first appeared around the time of puberty or later were disqualified from transition as minors. The requirement that gender dysphoria worsen during puberty was a critical diagnostic criterion.
¶ 25. 4. No significant mental health problems. Youth with ongoing mental health issues, aside from mild depressive feelings, were excluded from transition as adolescents.
[26:43] HUNTER: “I want to emphasize two of these criteria. Early onset gender dysphoria was a requirement for transition. Early onset was described by the Dutch in one paper as gender dysphoria, quote, from toddlerhood, and there had to be no active mental health issues. Mental health problems excluded a teenager from transition.”
¶ 32. It should also be noted that the Dutch studies have poor applicability to currently presenting cases of youth gender dysphoria. To be eligible for medical transition, patients had to have persistent gender dysphoria “from toddlerhood onwards” with clear cross-sex identification. Currently, most gender dysphoric youth are gender-normative until their teen years and present with a high burden of comorbid mental health conditions present before the onset gender dysphoria. These two factors would have rendered most of the youth seeking to transition today ineligible for transition using the Dutch protocol criteria. Therefore, it can be argued that the Dutch research should never have been used as justification for scaling the practice of pediatric gender transition widely.
[27:11] HUNTER: “The very patients the Dutch excluded, late-onset post-pubertal gender-dysphoric youth with comorbid mental health issues, are now the majority of youth being transitioned. We are transitioning the very population the Dutch excluded, excluded because they feared harm. Affirmative care with transition is now touted as the cure for mental health problems. Just eight years ago, mental health problems excluded someone from transition. Our profession has abandoned the Dutch criteria, and these criteria were never based on hard evidence, only good intentions.”
¶ 12. The community standard approach to care for distressed youth enables clinicians to use evidence-based approaches aimed at reducing severe distress and improving general functioning, while allowing for the possibility of medical transition in the future, once mental health symptoms are well managed, and the individual becomes a mature adult capable of consent. The ability to consent is particularly important as many “gender-affirming” interventions are associated with significant risks to health including risks that are harder to comprehend and appreciate until one becomes a mature adult— such as the loss or impairment of fertility and/or sexual function. […]
¶ 30. 9. Assessment of the ability to consent and understand risks. The Dutch researchers emphasized the need for young people to be able to provide meaningful consent, since the intervention is associated with known adverse effects such sterility, infertility, and a range of anticipated health risks from lifelong administration of cross-sex hormones.
[31:19] HUNTER: “For those that conduct future research in this area of medicine, the following questions must be answered: Can minors consent to transition? Can minors with active mental health problems consent? Can this research with hormones and surgery be done safely and ethically, when we know these treatments have negative effects on normal physiology, when these treatments probably have negative effects on an adolescent’s psychosocial development and their neurodevelopment, to include their executive decision-making? Can research with hormones and surgery be done safely and ethically when we know these treatments will lead to loss of sexual function, when we know these treatments will lead to infertility?”
Notably, Hunter uses the term “the community standard of care” to refer to an undefined practice standard in opposition to gender-affirming care:
[33:11] HUNTER: We need to return to the community standard of care for treating distress, and that is psychotherapy: ethical, compassionate psychotherapy that respects the child’s experience. Let me say that again, ethical compassionate psychotherapy that respects the child’s experience. This is what Europe is doing, our colleagues in Great Britain, Sweden, Finland and elsewhere agree change is needed. Less harm needs to be done, safety and ethics need to prevail.
This phrase (also as “the community standard” and “the community standard approach to care”) appears in paragraphs 2, 12, and 48 of SEGM’s letter:
¶ 2. There are currently two competing models of care for gender dysphoria. The “gender-affirming” model, which conceptualizes young people presenting with gender dysphoria as “transgender youth” and focuses on the provision of hormones and surgery for those seeking gender transition (not all transgender-identifying youth seek to medically transition, but many do). Over the last several years, this model of care gradually supplanted the previous community standard of care, which is based on a holistic view of identity formation, recognizing that identity undergoes changes during the adolescent and young adult years. This developmentally informed view recognizes that gender dysphoria can have many causes and many paths to resolution and does not support the notion that current gender identity should be medicalized into permanence using hormones and surgery in young people. Instead, psychotherapy is considered the first line of treatment, and gender transition in youth is pursued only in rare instances, as a measure of last resort. […]
¶ 48. Fifth, the Board should consider that the European countries that no longer medicalize youth gender dysphoria with hormones and surgery are treating it instead with psychological and psychiatric care. The Board should make a strong and unambiguous statement that psychotherapy for gender-related distress is the community standard and should not be stigmatized or conflated with conversion therapy.
Although Hunter and SEGM have called for a return to this alleged previous standard, the meaning of “the community standard of care”, in the context of opposition to gender-affirming care, is unusually elusive for a supposedly widespread and accepted practice predating affirmation. In the general context of transition treatments, “community standard of care” is typically used in discussions on ensuring access to transition care and other medically necessary care for trans people in carceral settings or other institutions; it does not appear to refer to any intended prohibition on trans youth or adults accessing any gender-affirming care (Kendig & Rosseau, 2022; Brief of amici curiae civil rights & non-profit organizations in Edmo v. IDOC, 2019; Washington State DCYF Policy 4.30 statement 11, 2018; Complaint and jury demand in Hill v. BOP, 2013).
SEGM’s use of this phrase, in opposition to any access to gender-affirming medical treatment by a significant portion of the transgender population, namely trans youth, appears to be novel. “Community standard of care” first appeared on SEGM’s FAQ page under “Why is there a ‘GIDS’ graph” (“Frequently Asked Questions”, retrieved on December 1, 2022) some time after October 18, 2022 (compare “FAQ”, Internet archive capture, October 18):
NHS England determined that the first line of treatment for youth gender dysphoria should be psychotherapy. The NHS concluded it’s not viable or safe to place the care for gender dysphoric youth in a “gender clinic” led by “gender experts.” Going forward, gender-dysphoric youth will be taken care of in standard clinical settings, led by experts in mental health, autism, child and adolescent development, trauma, and other relevant areas of expertise. The NHS decision has put an end to the “gender-clinic” model of care that is built on the foundation of “gender affirmation” endorsed by WPATH, and returned to the previous community standard of care based on a holistic view of identity development in children and adolescents.
This passage was not present in the October 18 version of SEGM’s FAQ, which primarily referred to the “standard of care” in the context of grounds for malpractice lawsuits against providers of transition treatments:
What is the standard of care in pediatric gender medicine?
There is much confusion about the “standard of care” in gender medicine. Standard of care is a medicolegal concept essential for determining whether clinicians are negligent and liable for their actions in the context of malpractice lawsuits. For example, if a certain treatment harmed the patient, but the doctor only did what any other competent and skilled doctor would do in a similar situation, the doctor’s attorney will assert that they practiced according to a standard of care and should not be liable, even if the patient was demonstrably harmed.
What is contributing to the confusion is that an organization that promotes the practice of “gender-affirmation” of youth with hormones and surgeries, The World Professional Association for Transgender Health (WPATH), named their treatment guidelines “Standards of Care” also known as “SOC.” In a recent court case, WPATH clarified that despite the misleading name, their practice guidelines are indeed treatment recommendations and not a “standard of care.”
Ultimately only the courts can determine whether clinicians who provide “gender-affirming” interventions can successfully invoke the standard of care argument when sued by a patient alleging harm. Those who will argue for it will point out that currently a number of medical organizations have embraced the practice of “gender affirmation” following WPATH’s treatment recommendations. However, such an argument may not withstand scrutiny due to two key facts: the evidence base for “gender-affirming” interventions, as well as the WPATH guidelines themselves are recognized to be of very low quality; and a growing number of healthcare systems in the Western world recently diverged from WPATH recommendations, sharply limiting pediatric gender transitions to a few exceptional cases.
This does not actually describe or propose the substantial components of any such standard of care or how this would differ from existing gender-affirming care. SEGM’s post-October 18 FAQ refers to SEGM’s own October 24, 2022 blog post “The NHS Ends the ‘Gender-Affirmative Care Model’ for Youth in England”, which states:
The key highlights of the NHS new guidance are provided below.*
1. Eliminates the “gender clinic” model of care and does away with “affirmation”
The NHS has eliminated the “gender clinic” model of care where children are seen solely by a specialist gender dysphoria practitioner, replacing it with standard care in children’s hospital settings.
This post links to NHS England’s October 20 “Interim service specification for specialist gender dysphoria services for children and young people – public consultation” , which includes the documents “Public consultation”, “Interim service specification”, and “Equality and Health Inequalities Impact Assessment (EHIA)”. However, none of these documents include references to any “community standard of care” as used by SEGM. In particular, the October 20 interim service specification features key differences from SEGM’s recommendations in their October 27 letter to the Boards. SEGM called to “discourage early social transition” with “no medical interventions before age 12” (paras. 22-23):
¶ 22. 1. Discourage early social transition. The Dutch clinicians recognized that early gender transition creates a stressful environment for children as they reach adolescence, should they wish to detransition. At the time it was widely acknowledged (and is still acknowledged by the current Endocrine Society guidelines) that most gender dysphoric children will not identify as transgender by the time they reached adulthood. It was also noted that even for those who would go on to transition, early social transition creates unrealistic expectations and subsequent disappointment with the natural limits of transition-related healthcare.
¶ 23. 2. No medical interventions before age 12. For prepubertal and early-puberty children <12 years, the Dutch standard of care was watchful waiting, careful observation, and psychotherapy if needed.
However, the NHS interim service specification allows for youth to continue a current social transition to maintain their level of functioning, initiate a social transition to maintain or improve their level of functioning, and begin treatment with puberty blockers at Tanner stage 2 if eligible:
In cases where a pre-pubertal child has effected, or is effecting, a social transition (or expresses a wish to effect a social transition) the clinical approach has to be mindful of the risks of an inappropriate gender transition and the difficulties that the child may experience in returning to the original gender role upon entering puberty if the gender incongruence does not persist into adolescence.
However, some children state that they want to make a social transition to their preferred gender role long before puberty, which means that increasing numbers of children may have made a partial or full social transition prior to the first attendance with The Service.
In summary, for pre-pubertal children the clinical approach and advice applied by The Service will be supportive and non-judgemental, balancing on a case-by-case basis a watchful approach overall with a more individualised approach in cases where the child’s level of global functioning may be maintained or improved through a carefully observed process of exploration of social transition. Medical interventions will not be considered at least until puberty has been reached (Tanner Stage 2).
Hunter and SEGM have represented an anti-trans “community standard of care” as a previously established and widespread historical practice, when this appears to refer instead to a set of mere assertions by SEGM – which are not practice standards – first published in a letter on October 27, 2022. Additionally, even though SEGM’s letter is dated prior to the October 28 meeting, it was not uploaded to the public book PDF until the day before the November 4 hearing, leaving the public with almost no time to review SEGM’s submission prior to BOM member Hunter’s extensive unattributed use of this third-party work. It is still not established at all whether there is any such earlier anti-trans “community standard of care” to which providers can “return”: it is apparently conjured from a network of mutual citations, with no ultimate reference to the substance of this alleged standard. Notably, the term “community standard of care” later appeared in a November 8 letter by SEGM to Iceland’s Althing parliament on the proposed Conversion Practices Prohibition Bill:
The low certainty of benefit of hormone treatments of youth was also reached by a recent “overview of systematic reviews” commissioned by the U.S. State of Florida (Brignardello-Peterson & Wiercioch, 2022). In November 2022, Florida’s Medical Board determined that hormones and surgeries for gender dysphoric youth are experimental, and banned this practice in general medical settings (Ghorayshi, 2022). The Board encouraged clinicians to treat gender dysphoric youth under the well-established “community standard of care” for distress, which is psychotherapy. […]
In Iceland, no diagnosis appears to be required to initiate social transition of minors, and clinicians are advised to refer for puberty blocking medication. To the best of our knowledge, many health practitioner codes of practice already follow this rubric. According to the Bill, should clinicians in Iceland follow international developments and the conventional standard of pursuing noninvasive interventions before attempting medication and surgery, making a referral to psychotherapy would in effect be considered practicing “conversion.”
In this instance, SEGM is not quoting the BOM broadly but BOM member Hunter specifically, who himself appeared to be quoting SEGM’s previous October 27 letter. Within these two SEGM letters, this “community” or “conventional” standard of care is not detailed, consisting largely of negative statements and prohibitions on most gender-affirming approaches and treatments. However, SEGM twice acknowledges the possibility that these “community standard” practices could be found to fall under definitions of anti-gay and anti-trans conversion therapy. The group’s alleged “community standard of care” altogether does not appear to consist of anything more than possible conversion therapy (as “conversion therapy” is understood by those who are not members of SEGM). Conversion therapy practices are recognized by the United Nations as a cruel, inhumane, degrading, and profoundly traumatic human rights violation, and can be considered an act of torture against LGBT people (“One UN human rights expert’s fight to eliminate ‘conversion therapies’”, UN News, February 18, 2022).
Hunter’s introduction of an alleged “community standard of care” was inappropriately vague, did not properly attribute SEGM’s October 27 letter, and did not disclose details relevant to the public health mission of the BOM; namely, the risk that this vague standard could overlap with conversion therapy practices considered to be highly dangerous and harmful to trans youth. Instead, Hunter has allowed Florida’s state health agencies to be used as a mouthpiece for the outside interest group SEGM, laundering their poorly-articulated and risky proposals via the Boards to be exported abroad with apparent authority.
5. BOM member Patrick K. Hunter has a history of failing to disclose significant and relevant information about his qualifications in bioethics
In his May 2022 expert declaration in Eknes-Tucker et al. v. Ivey et al., BOM member Dr. Patrick K. Hunter stated that he is a “pediatrician with an advanced degree in bioethics” awarded by the University of Mary in 2020. Declaration of Patrick Hunter, May 1, 2022:
1. I submit this expert declaration based upon my personal knowledge, my experience as a pediatrician with an advanced degree in bioethics, and my review of the literature discussed below. […]
3. I am a pediatrician with a master’s degree in bioethics. I received my medical degree from the University of Louisville School of Medicine in 1992 and completed a pediatric residency at Tripler Army Medical Center in 1995. I obtained board certification in general pediatrics in 1995 and have continuously maintained that certification. I obtained a Master of Science degree in bioethics from the University of Mary in 2020. I have served on the ethics committee at Nemours Children Hospital, Orlando. […]
The Master of Science degree in bioethics from the University of Mary is not merely an “advanced degree in bioethics”, but a degree focused entirely on a specific Catholic interpretation of bioethics (“Bioethics, M.S. – University of Mary”). The University of Mary describes the program’s Catholic focus:
Bioethics is broadly interdisciplinary and encourages collaboration of various stakeholders in the discourse that helps people make morally sound decisions made within our Christian, Catholic, and Benedictine tradition, about responsible use of biomedical advances. […] Informed by the Christian, Catholic and Benedictine tradition, the program in Bioethics prepares graduates to meet bioethical health care challenges with confidence, courage and clarity.
One pathway for this degree is offered in association with the National Catholic Bioethics Center, an “allied organization” of the Catholic Medical Association:
The interdisciplinary Master of Science in Bioethics Degree offered in partnership with the National Catholic Bioethics Center (NCBC) consists of 32 credits and can be completed in two years. In the first year, the student enrolls in the NCBC Certification Program in Health Care Ethics.
All pathways for the M.S. in Bioethics are based on the NCBC’s teachings: Year one of the University of Mary M.S. in bioethics requires either the “NCBC Certificate Courses”, or attending “HCB 550 – NCBC Two-Day Bioethics Seminar”. Like the Catholic Medical Association, NCBC holds specific absolute positions on the topic of ethical care for trans youth, and opposes any affirming care or transition treatment for trans youth as well as adults. The group broadly describes all aspects of transitioning as “always morally evil” on the grounds of “Catholic anthropology and Church teaching”. In the NCBC’s 2021 book “Transgender Issues in Catholic Health Care” (Furton, 2021), NCBC Staff Ethicist Josef P. Zalot contributed the chapter “Catholic Health Care and Gender Identity: A Resource for Policy Guidance”, writing:
The affirmative model of care fails the principle of double effect on at least two of the four criteria. The first is criterion 1. To determine the liceity of a particular action (or intervention), one needs to evaluate it in light of the moral object – that which gives the act its moral significance. When psychotherapy is used to affirm patients’ perceptions that they are in the wrong body, to encourage them to socially transition, and then to move them toward hormones and surgical procedures, the moral object is gender transition – understood as the deliberate alteration of a person’s thinking, behavior, or appearance to affirm that person’s erroneous perception of sexual identity. Similarly, when puberty-blocking hormones are prescribed (and provided) for the direct and intended purpose of offering a child more time to discern his or her so-called true sex, the moral object is gender transition. When cross-sex hormones are prescribed (and provided) for the direct and intended purpose of altering one’s secondary sex characteristics (breasts, facial hair, and so on) so that the body presents with the physical attributes of one’s preferred gender, the moral object is gender transition. As previously explained, transitioning one’s gender (or attempting to do so) is contrary to Catholic anthropology and Church teaching, not to mention logic, basic biology, and medical evidence. As such, interventions directed toward this end are never morally good or neutral; they are always morally evil.
Notably, Hunter explains in his May 2022 declaration that the focus of his bioethics degree was “ethical dilemmas” presented by gender-affirming care:
15. I have always had a keen interest in medical ethics and often considered formal education in the field. I originally wanted to explore the merging of medicine and business—hospital systems dominating the marketplace and physicians becoming employees—and how this evolution was impacting the ethics of medical care. What I was learning about gender dysphoria further propelled my interest in an ethics degree. I undertook a study of bioethics, completing my master’s degree in bioethics in 2020.
16. In my degree, much effort was focused on the growing popularity of the so-called “gender-affirmative care,” which delivers life-altering, permanent interventions to minors that involve sterilizing procedures. I have focused on ethical dilemmas, such as whether minors have the capacity to give a meaningful informed consent.
According to the NCBC, which plays a foundational role in this bioethics program, the “ethical dilemma” of gender affirmation is clear: it is “always morally evil”. This directly comes to bear on BOM member Hunter’s statement at the November 4 meeting calling for “ethical, compassionate psychotherapy”. The NCBC states outright that “[w]hen psychotherapy is used to affirm” trans people’s genders, or when “the moral object is gender transition”, it is “morally evil”. This judgment of gender-affirmative care as “evil” is attributed to teaching and “anthropology” that is particular to this group’s interpretation of one religious faith.
BOM member Patrick K. Hunter has a documented history of adhering to a narrow religious view of bioethics as applied to care for trans youth. It is not clear why these sectarian interpretations of bioethics would be of any relevance to the citizens of Florida impacted by the proposed Rules; the vast majority of Floridians, 79%, are not Catholic (2014 Religious Landscape Survey, Pew Research Center). In any case, these positions based on one group’s religious doctrine have no place in any policymaking under the secular government of the United States.
Hunter should have disclosed that his approach to medical ethics is heavily informed by non-mainstream sectarian religious views and policies promoted by outside influence groups, which are not shared by most Floridians. Members of the Boards should be required to disclose any such deviancy in their training and credentials in medical ethics from mainstream standards of ethics and core public health goals. The Boards must prioritize the overall public health mission of Florida’s state health agencies and promote the health and well-being of all Floridians regardless of their religious faith or life philosophy.
6. State-selected anti-trans expert Michael Biggs misleadingly conflated two distinct groups when describing transition outcomes
At the October 28 joint Boards meeting, anti-trans expert Michael Biggs made the misleading claim that a patient “died as an indirect consequence of puberty suppression” when this was a postoperative complication of vaginoplasty:
[32:49] MICHAEL BIGGS: De Vries et al. acknowledge that one patient was killed by necrotizing fasciitis during vaginoplasty, out of 70 patients that’s a death rate exceeding 1%, remarkably high for a group of healthy teenagers. De Vries et al. didn’t mention that the death was actually a consequence of puberty suppression, as I’ll explain in a moment.
[. . .]
[34:25] Well, it’s certainly true that early puberty suppression produces a closer resemblance to the opposite sex, patients are more likely to pass superficially. However, this benefit must be weighed against several serious costs. There are some known costs. So for males, early puberty suppression makes subsequent genital surgery more risky and less satisfactory. The penis is so undeveloped that a normal vaginoplasty is usually impossible, and so instead a portion of the patient’s intestine has to be used. Leakage from the intestines after surgery is what killed the early Dutch patient at the age of 18, so that patient died as an indirect consequence of puberty suppression. [35:08]
Biggs is a sociologist and does not specialize in the treatment of gender dysphoria in youth. Biggs also did not note the limitation that because this study’s sample size is less than 100, the occurrence of any one rare event would result in the “rate exceeding 1%” that he considers “remarkably high”. He additionally erred in conflating two groups that are not comparable: patients receiving puberty blockers for gender dysphoria, and patients receiving intestinal vaginoplasty.
Both of these groups are heterogeneous. The group of those receiving puberty blockers for gender dysphoria includes those assigned female (a possible majority) who would not receive any vaginoplasty, those assigned male who later undergo intestinal vaginoplasty, those assigned male who later undergo non-intestinal vaginoplasty, and those assigned male who do not undergo any vaginoplasty. Contrary to Biggs’ assertion, van der Sluis et al. (2022) found that 28% of assigned-male trans youth using puberty blockers since Tanner stages 2-3 were able to receive non-intestinal penile inversion vaginoplasty.
The group of patients undergoing intestinal vaginoplasty is also heterogeneous, including cisgender women with various conditions of the reproductive tract, trans women without a history of using puberty blockers, and trans women with a history of using puberty blockers. Bouman et al. (2014) found in a review of intestinal vaginoplasty outcomes that “procedure-related complication rates were low” and “only 0.6% of patients had severe procedure-related complications”. Because Biggs is discussing a complication with intestinal vaginoplasty, this concern would not be applicable to those using puberty blockers who do not undergo this procedure.
Biggs erroneously presented those using puberty blockers and those receiving intestinal vaginoplasty – two very different groups – as effectively synonymous when they are not even directly comparable due to their distinct compositions with limited overlap. However, the Boards failed to challenge these inaccurate assertions at the time they were made. Biggs’ remarks on these outcomes should be excluded by the Boards from consideration as expert testimony.
7. State-selected anti-trans expert Dr. Michael K. Laidlaw incorrectly described desistance of gender dysphoria as occurring at adulthood rather than adolescence
At the October 28 meeting, anti-trans expert Dr. Michael K. Laidlaw presented a slide (Oct. 28 public book version D, p. 137) claiming that the “desistance of children by adulthood” is “50-98%” and attributing this to Ristori & Steensma (2016):
[1:36:27] DR. MICHAEL K. LAIDLAW: I think it’s important to note that studies have shown that desistance, or growing out of this condition of children by adulthood, is very high, some 50 to 98%, and these are primarily studies done on 12 years old and younger.
[Slide stating “Desistance of Children by adulthood: 50-98%*”, citing Ristori & Steensma (2016).]
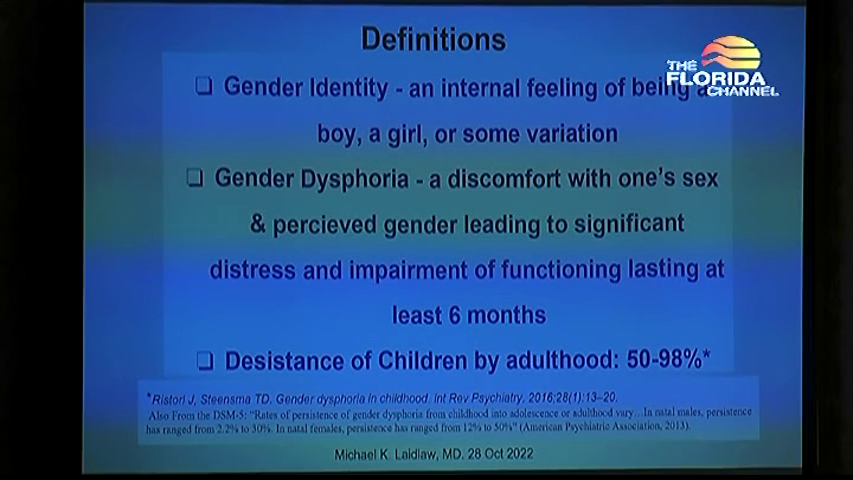
However, Ristori & Steensma specify that ages 10-13 are a crucial developmental period for the divergent outcomes of desistance or persistence – not adulthood:
The primary aim of the Steensma et al. (2011) study was to get a better understanding of the processes that contribute to the persistence and desistence of childhood GD. By interviewing adolescents (14 persisters, 11 desisters) who all fulfilled the DSM-IV or DSM-IV-TR criteria of a gender identity diagnosis in childhood (APA, 1994, 2000), it became clear that the period between 10 and 13 years was considered crucial. Both persisters and desisters stated that the changes in their social environment, the anticipated and actual feminization or masculinization of their bodies, and the first experiences of falling in love and sexual attraction in this period, contributed to an increase (in the persisters) or decrease (in the desisters) of their gender related interests, behaviours, and feelings of gender discomfort.
Ristori & Steensma also note a previous finding that persistence rates increased over time as some trans patients, who had apparently “desisted” as youth, later returned to the clinic as adults:
To test this hypothesis, Steensma & Cohen-Kettenis (2015) recently published a report on the first 150 childhood cases from Amsterdam, the Netherlands, and checked whether a longer follow-up period would result in higher persistence rates. The children were at the time of first assessment – between 5 to 12 years old and between 19 to 38 years of age at the time of follow-up. Out of the 150 cases, 40 re-entered the clinic during adolescence (12–18 years of age) and turned out to be persisters (26.7%). However, after checking the files of the adult clinic (which sees nearly all adults with gender dysphoria in the Netherlands), it appeared that five individuals applied for treatment after the age of 18, raising the persistence rate to 30% and showing the importance of long-term follow-ups. Based on this information, it seems reasonable to conclude that the persistence of GD may well be higher than 15%.
Laidlaw’s argument gives the inaccurate impression that waiting beyond adolescence and into adulthood is necessary in order for “desistance” to occur, which is not supported by the cited paper. Laidlaw’s testimony also conspicuously failed to address the impact of the Boards’ proposed total ban on up to 50% of gender-dysphoric children, who will (as Laidlaw himself recognizes) continue to experience gender dysphoria throughout their adolescence and into adulthood.
Because a copy of Ristori & Steensma (2016) including these passages was enclosed in the August 5 public materials (pp. 10-17), members of the Boards should have been aware of these key details. Instead, the Boards failed to challenge Laidlaw’s incorrect statements at the time they were made. Laidlaw’s remarks on desistance should be excluded by the Boards from consideration as expert testimony.
8. BOM member Dr. Patrick K. Hunter incorrectly argued that social transition is causative of persistence of gender dysphoria
At the October 28 meeting, BOM member Patrick Hunter argued that social transition “changes the desistance rates” and that youth who socially transition “would then need to understand the surgical risks” (see Appendix A, 4:46:28):
[4:47:14] DR. PATRICK K. HUNTER: But any informed consent needs to disclose the degree of evidence or lack thereof, whether that, who that’s coming from. I agree it needs to be a multi-disciplinary process. That’s what the Dutch said they would do, and that needs to be, it’s the, informed consent is not a simple process in this setting. It has to include surgery. I think it needs to include surgery, because once you’re on the path of social transition, there’s good, there is good evidence that social transition maintains that identity and it changes the desistance rates.
[4:47:53] Once that’s started, then you’re on puberty blockers. We’ve heard that puberty blockers lead 98% chance [sic], 95% chance of cross-sex hormones. Now we’re in the irreversible territory. What percentage of those kids go on to surgery? So for a 12, 13, 14 year old to understand that, they would then need to understand the surgical risks, because they’re starting on a pathway that may not go back, that may be irreversible. So the consent process would have to involve a surgeon, I believe, too, for the family to understand. The 12 year old, 13, 14 year old might not understand that. But the parents, I think, are due that knowledge of what the evidence reviews show, and the full gamut of what may proceed over the next four, five, six years. [4:48:38]
This assertion of a causative mechanism is based on a misreading of Steensma et al. (2013), which proposed the authors’ own logistic regression model of predictive factors rather than causative factors (“Dr. Stephen Levine and the Plot to Police America’s Gender”, Gender Analysis, June 1, 2022). Even within this model, social transition status was one of multiple factors, and explained 12% of the outcome of whether an assigned-male child would experience persistence of their gender dysphoria into adolescence. For those assigned female, who may now comprise a majority of trans youth, social transition status was not even predictive of an outcome of persistence or desistance at all.
Because there is no indication that social transition causes persistence of gender dysphoria, this does not support the argument that social transition in trans children – a reversible non-medical step including a change of name, attire, pronouns or hairstyle – should require the same capacity for informed consent as an adult agreeing to gender-affirming surgery. BOM member Hunter should not have made these incorrect claims at the time of the October 28 meeting, and these statements should be excluded from consideration by the Boards.
9. BOM member Dr. Patrick K. Hunter introduced irrelevant and misleading arguments to amplify the credentials of AHCA GAPMS report authors Brignardello-Petersen and Wiercioch
At the October 28 meeting, BOM member Patrick Hunter offered this response to Yale School of Medicine’s Dr. Meredithe McNamara, following her criticism of the AHCA GAPMS report authors’ lack of relevant expertise in gender-affirming care:
[2:03:15] DR. PATRICK HUNTER: This is going to be more of a statement, but then I would like Dr. McNamara to comment. The concern seems to be with the June 2 report, and I just want to clarify that this is my reading of the June 2 report, my understanding of the June 2 report, this is not a Florida report. This is a report from McMaster University in Ottawa, Canada. And I agree those people who wrote the report are not physicians, they are not involved in gender medicine, but they are experts in evidence review, McMaster University being the home of the term “evidence-based medicine”. Gordon Guyatt coined that term, and these are all trainees of Dr. Guyatt.
[2:04:02] And I think there is some concern in the literature that if evidence is not reviewed in this systematic fashion, and if it is reviewed by people heavily involved in the field, that the conclusions may in fact be biased. So I don’t think there’s a bigger name in evidence-based medicine than McMaster University and the experts who reviewed the literature in this area. I just want that clear and for the record, and if Dr. McNamara would like to comment on that.
[2:04:37] DR. MEREDITHE MCNAMARA: I’m not sure if you’d like me to comment, but I really couldn’t hear much of what you said. I apologize if I’ve missed.
[2:04:47] HUNTER: I can try to say it again. I think to describe the evidence reviewers as inexpert and not qualified, when it’s coming from McMaster University, where the term “evidence-based medicine” [sic] and they have an entire program reviewing the quality of evidence. [2:05:10]
This diversion was irrelevant and a waste of the public’s time on these matters: Hunter’s argument fundamentally does not succeed in supporting the quality of the authors’ work. No particular institution holds a monopoly on evaluating medical evidence or basing decisions on scientific findings; this is antithetical to every value of the open processes of science. While Hunter’s statement reiterates Brignardello-Petersen & Wiercioch’s credentials, the issue at hand was the quality of the June 2 GAPMS report; extensive issues with their report are documented in the Yale School of Medicine’s submission to the BOM (“Public comments on Florida proposed rule denying Medicaid coverage for gender-affirming medical care”, July 8, 2022).
Although Hunter represents the authors as experts in evidence review, Brignardello-Petersen & Wiercioch failed to note a critical limitation of their June 2 review: the unavoidable bias present in a majority of the AHCA’s expert reports, which were written by individuals with a prior commitment to find against gender-affirming treatment in all circumstances regardless of evidence. Their eminent credentials make this omission all the more inexplicable, and Hunter and other members of the Boards did not address whether it is routine practice at McMaster University to omit any accounting of these biases from evidence reviews.
Notably, although Brignardello-Petersen and Wiercioch have coauthored a number of evidence reviews and practice guidelines in a variety of medical subspecialties, these publications typically had 10 or more coauthors, and always included a number of specialists in the relevant medical fields. These include reviews and guidelines on:
- Sensitive teeth (Martins et al., 2020) (12 authors)
- Cavity treatment (Urquhart et al., 2019) (19 authors)
- Dental care in epidermolysis bullosa (Krämer et al., 2012) (10 authors)
- Allergic rhinitis and asthma (Brozek et al., 2017) (60 authors)
- Corticosteroids for sore throat (Sadeghirad et al., 2017) (9 authors)
- Treatment of gout (FitzGerald et al., 2020) (34 authors)
- Ulcer prevention in ICUs (Alhazzani et al., 2018) (21 authors)
- Management of von Willebrand disease (Connell et al., 2021) (19 authors)
- von Willebrand factor levels (Kalot et al., 2022) (23 authors)
- Cervical cancer screening (Mustafa et al., 2016) (15 authors)
- Treatment of premalignant cervical lesions (Santesso et al., 2016) (15 authors)
- Treatment of acute myeloid leukemia in older adults (Sekeres et al., 2020) (23 authors)
- Comparing treatments for acute myeloid leukemia (Chang et al., 2021) (19 authors)
- Ventilation in COVID-19 (Schünemann et al., 2020) (50 authors)
- Remdesivir in COVID-19 (Rochwerg et al., 2020) (27 authors)
- Adverse effects of COVID-19 treatments (Izcovich et al., 2021) (15 authors)
- Diagnosis of VTE (Lim et al., 2018) (17 authors)
- Treatment of VTE and PE (Ortel et al., 2020) (22 authors)
- Test accuracy in diagnosing VTE (Patel et al., 2020) (29 authors)
- Comparison of anticoagulants (Neumann et al., 2020) (17 authors)
- Anticoagulants in cancer patients (Lyman et al., 2021) (16 authors)
- Anticoagulants in COVID-19 (Cuker et al., 2021) (45 authors)
- Heparin-induced thrombocytopenia (Morgan et al., 2020) (13 authors)
Outside of the June 2 GAPMS report, they do not have a history of writing reviews or guidelines with only one or two authors. This report was clearly conducted outside of Brignardello-Petersen and Wiercioch’s normal procedures for evidence reviews. While SEGM in their October 27 letter encouraged BOM not to “do it alone” (para. 3), Brignardello-Petersen and Wiercioch appear to have done exactly that in a dramatic departure from the standards of their previous work. Members of the Boards should refrain from irrelevant commentary that inappropriately inflates the quality of inadequate state-commissioned expert reports by individuals working outside of their areas of practice.
10. The Boards accepted an imbalanced lineup of anti-trans detransitioners and other anti-trans speakers from the FLDOH, including several undisclosed witnesses for AHCA in Dekker v. Marstiller
At the November 4 meeting, BOM member Dr. Hector Vila moved to eliminate the clinical trial exemption for use of puberty blockers and HRT by trans youth, citing the testimony of nine anti-trans detransitioners at the previous October 28 meeting (see Appendix B, 20:35):
[22:04] DR. HECTOR VILA: And finally and most significantly, the in-person testimony of multiple patients who were irreversibly harmed by hormonal treatments. In my 25 years of hearing testimony before this Board, I don’t think I’ve ever seen that many patients talk about that much harm being done to them. And so given these facts, I am not supportive of this, of item 2 in the proposed rule, that allows for these treatments to be administered under even IRB-approved protocol. I just don’t think that they’re safe, and that they cause irreversible harm to a significant number of patients.
Vila has mistaken repetition for abundance, misrepresenting these anti-trans detransitioners as prolific, when they are actually rare but frequently resampled. Notably, although the October 28 meeting featured testimony from nine of these detransitioners, the Florida Board of Medicine has previously suspended the license of a Boynton Beach doctor in 2017 who had prescribed opioids, benzodiazepines, and other medications linked to 4 patient deaths (“Boynton Beach doctor’s license suspended over 4 patient deaths”, South Florida Sun-Sentinel), and the Florida Department of Health suspended a Lake City prescriber in 2011 linked to 34 deaths from overdose (“Florida Pain Doc Suspended; 34 Patients Dead”, ABC News). The harms alleged by these nine anti-trans detransitioners are not singularly severe over the past 25 years of state supervision of medical practice in Florida, and many of these detransitioners received transition treatment and gender-affirming care outside of Florida.
The small group of detransitioners at the October 28 meeting have been reused for their anti-trans testimony by the AHCA in 2022 in Dekker et al. v. Marstiller et al. and in other anti-trans efforts outside of Florida over the past several years:
- [3:17:28] Detransitioner Zoe Hawes, who also provided a declaration for the state of Florida’s defense of AHCA’s transition care exclusion in Dekker et al. v. Marstiller et al. (Declaration of Zoe Hawes, October 3, 2022)
- [3:23:22] Detransitioner Chloe Cole, provided a declaration in Dekker v. Marstiller (Redacted defendants’ response in opposition, October 3, 2022) and offered anti-trans testimony to California and Louisiana state legislatures (“Chloe’s story: puberty blockers at 13, a double mastectomy at 15”, MercatorNet).
- [3:26:08] Detransitioner Camille Kiefel, provided a declaration in Dekker v. Marstiller (Declaration of Camille Kiefel, October 3, 2022)
- [3:32:03] Detransitioner Clifton Francis (Billy) Burleigh, also contributed to an amicus brief for the defense of Alabama’s trans youth care ban in Eknes-Tucker v. Ivey (Brief for amici curiae detransitioners, July 5, 2022), contributed testimony to the defense of Arkansas’ trans youth care ban in Brandt et al. v. Rutledge et al. (Brief of defendants-appellants, November 12, 2021), and testified in support of proposed trans youth care ban H.675 in Idaho (House State Affairs Committee minutes, March 4, 2022)
- [3:38:24] Detransitioner Helena Kerschner, contributed to an amicus brief in Eknes-Tucker v. Ivey
- [3:41:31] Detransitioner Ted Halley, contributed to an amicus brief for the defense of Alabama’s trans youth care ban in Eknes-Tucker v. Ivey
This was not the tip of an iceberg of such cases, but a small recurring cast of characters who are frequently resampled for lack of any broader testimony as to the prevalence of this allegedly widespread and concerning phenomenon. Three other speakers at the October 28 Boards meeting have been reused by the AHCA and in other anti-trans efforts:
- [3:45:00] Parent Yaacov Sheinfeld, provided a declaration in Dekker v. Marstiller (Declaration of Yaacov Sheinfeld, October 3, 2022), also contributed a brief in Eknes-Tucker v. Ivey (Declaration of Yaacov Sheinfeld, April 29, 2022) and contributed a brief in Brandt v. Rutledge (Brief for Yaacov Sheinfeld et al as amici curiae in support of defendants-appellants, November 19, 2021)
- [4:06:38] Dr. Robert Roper, physician of detransitioner witness C.G. who provided a declaration in Dekker v. Marstiller (Redacted defendants’ response in opposition, October 3, 2022)
- [4:18:20] Parent Bob Framingham, husband of Julie Framingham who provided a declaration in Dekker v. Marstiller (Declaration of Julie Framingham, October 3, 2022)
The public comment period of the October 28 meeting altogether featured 15 anti-trans speakers and only 6 pro-trans speakers. During the October 28 meeting, the Boards demonstrated undue deference to these anti-trans speakers, inconsistent with their standards of civility and decorum applied at other meetings. Anti-trans speaker Kiefel (Appendix A, 3:26:08) was permitted to attack the bodies of an identifiable group, transitioned Floridians, as being “mutilated”, “carved-up” and unlovable specifically due to undergoing these treatments; at no point did the Boards interrupt this inappropriate and prejudiced commentary. The following week at the November 4 meeting, pro-trans speaker Kimberly Cox (Appendix B, 1:31:19) was cut off and removed by BOM chair Dr. David Diamond for referring to the DeSantis administration as a “Nazi regime”. The Boards’ approach to civility is being applied in a way that silences pro-trans voices while elevating anti-trans voices, giving the impression that criticism of an autocratic approach to policymaking is unacceptable, while intrusive attacks on the bodies of thousands of trans Floridians are welcome.
On October 28 following the joint meeting, BOM member Dr. Zachariah P. Zachariah stated to Florida Politics that he “read the names in the order they were given to him by Department of Health staff” (“Medical board members have Gov. DeSantis’ back financially and on gender-affirming care”, Florida Politics, October 28, 2022). The Boards broadly, BOM chair Dr. David Diamond, and BOM member Dr. Zachariah P. Zachariah should have disclosed prior to the hearing that this lineup was provided by the Florida Department of Health. They should have rejected this imbalanced lineup of 15 anti-trans speakers and 6 pro-trans speakers. They should have additionally disclosed the affiliations of anti-trans speakers Zoe Hawes, Chloe Cole, Camille Kiefel, Yaacov Sheinfeld, Dr. Robert Roper, and Bob Framingham with the AHCA’s defense in Dekker et al. v. Marstiller et al. Members of the Boards should refrain from misrepresenting the population of anti-trans detransitioners as larger than it is.
The lineup of speakers at the November 4 joint meeting, which was described by BOM chair Dr. David as being “randomized” (see Appendix B, 19:33), featured both Zoe Hawes and Helena Kerschner again, as well as other anti-trans speakers linked to AHCA, FLDOH and other proposed care bans:
- [1:09:49] “Former trans kid” Erin Brewer, also testified in support of Idaho H.675 with Burleigh, and appeared at the October 28, 2021 “Virtual SAFE Act Summit” on Arkansas’ trans youth care ban with bill sponsor Rep. Robin Lundstrum (Response in opposition to motion to quash, Exhibit 15, in Brandt v. Rutledge, May 24, 2022)
- [1:19:59] Julie Framingham, provided a declaration in Dekker v. Marstiller (wife of Bob Framingham) (Declaration of Julie Framingham, October 3, 2022)
- [1:46:36] Parent Amy Atterberry, who stated in the November 4 public materials version Y (pp. 2308-2309) that she shared her now-adult trans child’s medical records with state surgeon general Joseph Ladapo, and appears to have been quoted by AHCA as “Katie Caterbury” in Dekker v. Marstiller (Redacted defendants’ response in opposition, October 3, 2022)
Arkansas Rep. Robin Lundstrum, who frequently emails with Erin Brewer (Response in opposition to motion to quash, Exhibit 14, in Brandt v. Rutledge), recognizes the likely outcome of trans youth care bans such as Arkansas’ “SAFE Act” and Florida’s Rules 64B8-9.019 and 64B15-14.014. At the July 22, 2021 Family Policy Alliance “Gender Issues Policy Panel” (Response in opposition to motion to quash, Exhibit 27), Lundstrum openly acknowledged that the passage of these bans would certainly be followed by the plausibly attributable deaths of trans children who were not able to access gender-affirming care:
3. The Tough Stuff
a. One of the questions that kept coming up over and over again, even reverberating nationally, was “what about the children who are already undergoing ‘treatment’ with puberty-blockers and/or cross-sex hormones”? How do you both respond to that?
i. Robin: We’re not looking in the medicine cabinet; these drugs are already dangerous; once off drugs, suicide risk goes down, so this is critical to get children off of these medications; need care of a physician to help them work off the drugs; be prepared to be blamed when a child identifying as transgender commits suicide—it WILL happen
Such proposals, known even by their proponents to be an antecedent to children’s deaths, have no place in the policies of any Florida state health agency. This stands in opposition to any meaningful understanding of public health and clearly jeopardizes the safety and well-being of the children of Florida. The Boards should not provide a platform to this or any such sentiment. Members of the Board of Medicine and Board of Osteopathic Medicine must ask themselves this, both in their professional role and in their personal role as members of their communities: What would you do if someone was coming to your state to promote a policy they knew would cause the deaths of children?
Conclusion and recommended actions
We call on the Florida Board of Medicine and Florida Board of Osteopathic Medicine to hold a hearing on critical irregularities in the rulemaking process leading to the proposed Standards of Practice for the Treatment of Gender Dysphoria in Minors. We call on the Boards to repeal proposed Rules 64B8-9.019 and 64B15-14.014 F.A.C., or indefinitely postpone these rules from taking effect until they can be appropriately revisited and repealed, on the grounds that these rules were not validly enacted due to these procedural irregularities.
Zinnia Jones, Gender Analysis
Heather McNamara, Gender Analysis
December 2, 2022
Appendix A: Transcripts of October 28 joint Boards hearing
Detransitioner and defense witness Camille Kiefel in Dekker et al. v. Marstiller et al. describes trans people’s post-transition bodies as mutilated and unlovable (3:26:08 in meeting video)
[3:26:08] CAMILLE KIEFEL: My name is Camille Kiefel. I stand here before you today, Florida Board of Medicine, in hopes that you’ll make the right decision regarding transitioning children, and take greater consideration for adults. Prior to my transition, I had spent 20 years in mental health therapy with conventional modalities. I didn’t respond well to medications, saw a gender therapist, and had two rounds of transcranial magnetic stimulation therapy. I was diligent in wanting to heal, but nothing my doctors offered had healed me, because they always saw my issue strictly as a mental one.
[3:26:49] I was 30 and at the end of my rope when I transitioned. At the time, I believed I was non-binary. I struggled with severe mental illness and suicidal ideation. I had a trauma history. When I was in 6th grade, my best friend had been raped by her brother. Being a girl meant I was vulnerable. I started to present more masculine. This should have been a red flag, yet within months of requesting top surgery, it was performed on me. I developed complications after my surgery. There were many times when I didn’t know if I would make it through the night.
[3:27:26] If I made this mistake as an adult, a young girl could too. Not only did this surgery exacerbate my mental health issues, I now struggle with physical complications as well. Presenting and taking on another gender was a way for me to escape womanhood. Escape is not a valid way of dealing with trauma. You will have to deal with it eventually. I was able to work through these difficult emotions and improve my mental health through a holistic approach. I had physical health issues that had been previously overlooked. Had that been managed, I would have never gotten the surgery. The surgery was an abhorrent misdiagnosis. The goal of healthcare should always be to get to the root cause of the problem.
[3:28:12] Today I am more grounded than I have been in my entire life, but I am mutilated. Between my carved-up body and the physical complications, I often question if there is anything on the other side. Where my breasts were are hollow. I can never get them back. I can never fit a dress the same way again. I can never breastfeed. Who will love me? You know what keeps me going? Stopping this from happening to someone else. Thank you for your time, you will have a lot to consider, and I know you will make the right decision. [3:28:50]
Anti-trans speakers, partial list
- [3:17:28] Detransitioner Zoe Hawes
- [3:20:27] Detransitioner Rachel Foster
- [3:23:22] Detransitioner Chloe Cole
- [3:26:08] Detransitioner Camille Kiefel
- [3:29:03] Detransitioner ”Shape Shifter”
- [3:32:03] Detransitioner Clifton Francis (Billy) Burleigh
- [3:35:13] Detransitioner Cat Cattinson
- [3:38:24] Detransitioner Helena Kerschner
- [3:41:31] Detransitioner Ted Halley
- [3:45:00] Parent Yaacov Sheinfeld
- [4:06:38] Dr. Robert Roper
- [4:18:20] Parent Bob Framingham
BOM member Dr. Patrick K. Hunter claims that social transition causes persistence of gender dysphoria and argues that social transition in childhood requires capacity to consent to surgery as an adult (4:46:43 in meeting video)
[4:46:28] DR. ZACHARIAH P. ZACHARIAH: I have a question for Dr. Hunter. Dr. Hunter, you deal with these things. Do you think they should have a psychiatric evaluation or some psychiatrist involved in this decision-making?
[4:46:40] DR. PATRICK K. HUNTER: The level of mental health care, whether it’s psychology, psychiatry, I think that’s up for debate. One thing that I think that any consent needs to recognize and needs to share with the patient and the family is the level of evidence, and what the systematic reviews have shown. The NICE reviews out of England on puberty blockers and cross-sex hormones are the best English-language reviews. The Swedish reviews are only summarized in English, they have not been translated from the Swedish language to the English language, the full reviews.
[4:47:14] But any informed consent needs to disclose the degree of evidence or lack thereof, whether that, who that’s coming from. I agree it needs to be a multi-disciplinary process. That’s what the Dutch said they would do, and that needs to be, it’s the, informed consent is not a simple process in this setting. It has to include surgery. I think it needs to include surgery, because once you’re on the path of social transition, there’s good, there is good evidence that social transition maintains that identity and it changes the desistance rates.
[4:47:53] Once that’s started, then you’re on puberty blockers. We’ve heard that puberty blockers lead 98% chance [sic], 95% chance of cross-sex hormones. Now we’re in the irreversible territory. What percentage of those kids go on to surgery? So for a 12, 13, 14 year old to understand that, they would then need to understand the surgical risks, because they’re starting on a pathway that may not go back, that may be irreversible. So the consent process would have to involve a surgeon, I believe, too, for the family to understand. The 12 year old, 13, 14 year old might not understand that. But the parents, I think, are due that knowledge of what the evidence reviews show, and the full gamut of what may proceed over the next four, five, six years. [4:48:38]
Appendix B: Transcripts of November 4 joint Boards hearing
BOM chair Dr. David Diamond states that speakers will be chosen randomly (19:33 in meeting video)
[19:33] DR. DAVID DIAMOND: And as far as public comment is concerned, it’ll be randomized, meaning selected out of the hat, A-B A-B, until the public comment is completed.
BOM member Dr. Hector Vila introduces motion to strike clinical trial exception (20:35 in meeting video)
[20:35] DR. HECTOR VILA: Thank you. I want to echo those comments, I appreciate what the Board has gone through hearing testimony, extensive testimony, and then all of the letters that have been submitted that we’ve looked through. I was not at the rules committee meeting, but I watched the entire video of it, and that even further added to the body of knowledge and discernment that I’ve gone through.
[21:05] And after hearing extensive testimony from physician experts on the irreversible harm due to puberty blocker medications as well as the hormone therapy, and after testimony that other countries have restricted access to medications, after written testimony from the author of a study that found a significant percentage of patients who transition later choose to detransition and thus have a significant percentage that have suffered irreversible harm, given the lack of testimony from expert proponents of hormone therapy that there are adequate selection criteria that have sufficient specificity to avoid harm, and after testimony from expert proponents of these treatments that in fact they are relatively rare in minors and thus our rules would not substantially deviate from the care that they are providing, and finally and most significantly the in-person testimony of multiple patients who were irreversibly harmed by hormonal treatments. In my 25 years of hearing testimony before this Board, I don’t think I’ve ever seen that many patients talk about that much harm being done to them.
[22:23] And so given these facts, I am not supportive of this, of item 2 in the proposed rule, that allows for these treatments to be administered under even IRB-approved protocol. I just don’t think that they’re safe, and that they cause irreversible harm to a significant number of patients. Now if you want to do any research, I suggest that you move it to those minors that are already undergoing treatment if they, if we want to ask the legislature to provide the data, but I want you to know that I am not support [sic] and I would move to strike item 2 in the resolution. [23:16]
BOM member Dr. Patrick Hunter seconds Dr. Vila’s motion to strike item 2 and reads a statement into the record (23:46 in meeting audio)
[23:46] DR. DAVID DIAMOND: Dr. Vila, please?
[23:48] DR. HECTOR VILA: I move to strike item 2 in the proposed standard of practice for the treatment of gender dysphoria in minors.
[23:54] DIAMOND: Do I hear a second on the motion?
[23:56] DR. PATRICK HUNTER: Seconded.
[23:58] DIAMOND: There’s a second. It is now open for discussion on that motion.
[24:03] HUNTER: Dr. Diamond.
[24:05] DIAMOND: Yes, sir?
[24:09] HUNTER: I want to read this into the record. Dutch researchers pioneered youth transition for gender dysphoria. They published several papers culminating in a 2014 paper that described the outcome for 55 youths they transitioned. The Dutch protocol is now what we call affirmative care: puberty blockers, cross-sex hormones, and breast and genital surgeries. The Dutch protocol was deemed a success because the youth continued to function well after surgery. This affirmative model of care has spread wildly in the last eight years. The Dutch protocol is the foundation youth transition was built on. It is flawed, it is based on weak evidence. These are some of the problems with the Dutch study.
[25:16] Many concerns have been raised about its methodology. It was a case series, a small cohort of 55 teenagers. There was no control group. The follow-up period was only 18 months. This short period should be of concern. And most importantly, there has been no long-term data reported on these 55. The Dutch have been asked for their long-term data. In a June New York Times article, Dr. de Vries, the lead author, said the Dutch has [sic] lost contact with 50% of their early cohort. Dr. de Vries was interviewed on an American podcast in January. She made it clear that their patients’ lives are much more complicated than the original study’s outcome suggests.
[26:15] The Dutch, to their credit, were concerned about false transitions – transitions that would later be regretted. False transitions would be the worst possible outcome. Today we call that regret and detransition. The Dutch had inclusion and exclusion criteria hoping to limit false transitions. I want to emphasize two of these criteria. Early onset gender dysphoria was a requirement for transition. Early onset was described by the Dutch in one paper as gender dysphoria, quote, from toddlerhood, and there had to be no active mental health issues. Mental health problems excluded a teenager from transition.
[27:11] The very patients the Dutch excluded, late-onset post-pubertal gender-dysphoric youth with comorbid mental health issues, are now the majority of youth being transitioned. We are transitioning the very population the Dutch excluded, excluded because they feared harm. Affirmative care with transition is now touted as the cure for mental health problems. Just eight years ago, mental health problems excluded someone from transition. Our profession has abandoned the Dutch criteria, and these criteria were never based on hard evidence, only good intentions.
[27:59] Now we have objective unbiased systematic reviews, the most prominent being from Swedish and British experts. These systematic reviews tell us the evidence for youth transition is poor quality and with very low certainty for benefit. However, we are told that more and more evidence supports hormonal and surgical transition. The quality of this research is extremely questionable. I want to cite one recent example. In September just two months ago in JAMA Pediatrics, there was a study reported from Northwestern University in Chicago. 70 patients were compared, 36 had a double mastectomy and 34 did not. The patients ranged in age from 13 to 24 years. The authors concluded that mastectomy was beneficial and should not be delayed in youth. What led them to that conclusion? The finding that three months after surgery, a mere 90 days, the 36 patients, as young as 13, 14 and 15 years, were happy with their flat chests. And it was not just 36 that had surgery, it was 42. They lost nine percent of their surgical cases to follow up, nine percent in three months.
[29:37] It is absurd, meaningless to draw any conclusions after three months. This paper is indicative of the quality of research we have in this field, published in our most prestigious journals. We have a serious problem. The testimony last week from those who have detransitioned is evidence of that. Finland, Sweden and England have changed course. They recognize harms are occurring, that the evidence is poor, that the Dutch protocol should not have been adopted and scaled to the extent that it has. In our last meeting I suggested we carve out an exception for research. After much thought I can no longer support that idea. I do not believe the Board is authorized to regulate medical research. That authority lies with other federal and state agencies. The Board’s duty is to regulate the general practice of medicine, and we can do that, we should do that, and allow others to address research in this field.
[30:55] But I want to say something about human medical research. Ethical principles of human medical research were first articulated in the Nuremberg Code, then in the World Health Organization’s Declaration of Helsinki, and further described in the United States Belmont Report which followed the terrible revelations discovered with the Tuskegee syphilis experiments. For those that conduct future research in this area of medicine, the following questions must be answered: Can minors consent to transition? Can minors with active mental health problems consent? Can this research with hormones and surgery be done safely and ethically, when we know these treatments have negative effects on normal physiology, when these treatments probably have negative effects on an adolescent’s psychosocial development and their neurodevelopment, to include their executive decision-making? Can research with hormones and surgery be done safely and ethically when we know these treatments will lead to loss of sexual function, when we know these treatments will lead to infertility?
[32:19] These ethical questions are very important, but it is also critical that researchers ask why so many young people are suffering from gender dysphoria. Depending on the survey, between 2 and 10 percent of youth now describe themselves as gender diverse. Many are suffering and need help. Researchers need to ask why this is happening. Why has the incidence of gender dysphoria skyrocketed? We would ask this question for any other condition. These questions need to be answered not just by the medical profession, but by society at large. Children and youth with gender dysphoria are suffering, they need care, the best possible care, excellent care.
[33:11] We need to return to the community standard of care for treating distress, and that is psychotherapy: ethical, compassionate psychotherapy that respects the child’s experience. Let me say that again, ethical compassionate psychotherapy that respects the child’s experience. This is what Europe is doing, our colleagues in Great Britain, Sweden, Finland and elsewhere agree change is needed. Less harm needs to be done, safety and ethics need to prevail. I’m confident the Board of Medicine will do the right thing. [33:52]
Pro-trans speaker Kimberly Cox and exchange with BOM chair Dr. David Diamond (1:31:19 in meeting video)
[1:31:19] KIMBERLY COX: More importantly, to everybody out there that’s watching and all of the people in this room, if you’re a teen or an individual who is thinking about suicide because of this decision today, please know from this mother: You are loved, you are valued, and you are more than worthy. And the men and women that sit here and donate to people like Governor DeSantis and the Nazi regime that he has –
[1:31:47] [gavel bangs twice]
[1:31:48] DR. DAVID DIAMOND: No!
[1:31:50] COX: Absolutely! You let them talk about the Bible, you will let me talk about this.
[1:31:56] DIAMOND: She’s gone. Next.
[1:32:02] COX: I have 24 seconds left, and I will say that you can call 988 and talk to somebody. If you feel that your life is in danger, please make sure you reach out. Shame on all of you! Shame on all of you! I know everything about you!
[1:32:36] DIAMOND: Next is Zoe Hawes. We’re not going to have people calling one another Nazis in this room today.
Anti-trans speakers, partial list
- [1:02:13] Diane Gowski, president of the Florida Catholic Medical Association
- [1:09:49] “Former trans kid” Erin Brewer
- [1:19:59] Julie Framingham (wife of Bob Framingham)
- [1:26:52] Detransitioner Prisha Mosley
- [1:33:04] Detransitioner Zoe Hawes (also appeared at Oct. 28 meeting)
- [1:40:43] Detransitioner Helena Kerschner (also appeared at Oct. 28 meeting)
- [1:46:36] Parent Amy Atterberry
Appendix C: Excerpts from declaration of Mario Dickerson, November 4, 2021
Declaration of Mario Dickerson, executive director of Catholic Medical Association, in American College of Pediatricians et al. v. Becerra et al., November 4, 2021:
2. I serve as the Executive Director of the Catholic Medical Association (“CMA”). Given my involvement in CMA, I am familiar with the organization’s history, the issues confronting it, and the views of the organization and its members concerning various emerging issues, including the gender identify mandate at issue in this litigation.
3. CMA is the largest association of Catholic individuals in healthcare. CMA is a national, physician-led community that includes about 2500 physicians and health providers nationwide. […]
9. CMA’s mission is to inform, organize, and inspire its members, in steadfast fidelity to the teachings of the Catholic Church, to uphold the principles of the Catholic faith in the science and practice of medicine. […]
23. The Catholic Church teaches that each person must be respected in their conscience. “Man has the right to act in conscience and in freedom so as personally to make moral decisions. ‘He must not be forced to act contrary to his conscience. Nor must he be prevented from acting according to his conscience, especially in religious matters.’” Catechism § 1782 (citation omitted). […]
27. CMA and its members sincerely believe that sex is a biological, immutable characteristic. […]
29. They respect the dignity of the human person as an embodied true male or female. […]
33. These beliefs reflect scientific reality, as well as thousands of years of Christian anthropology, with its roots in the narrative of human origins that appears in the Book of Genesis, when “God created man in his own image . . . male and female he created them.” Gen. 1:27.
34. The Catholic Church teaches that men and women are created in two sexes with corresponding identities. (2) [2: See, e.g., Catechism § 2333, 2393; Pope Francis, Encyclical letter Laudato Si’ ¶ 155 (2015), https://www.vatican.va/content/francesco/en/encyclicals/ documents/papa-francesco_20150524_encicli ca-laudato-si.html.]
35. The Catholic Church thus opposes invasive and drastic medical interventions promoted by modern gender ideology. “Except when performed for strictly therapeutic medical reasons, directly intended amputations, mutilations, and sterilizations performed on innocent persons are against the moral law.” Catechism § 2297.
36. The Catholic Church also teaches this lived biological reality of two sexes creates various obligations for public authorities. Catechism § 1907.
37. The Catholic Church’s most extensive statement today exclusively on gender identity is Male and Female He Created Them: Towards a Path of Dialogue on the Question of Gender Theory in Education. (3) [3: Congregation for Catholic Education, Male and Female He Created Them: Towards a Path of Dialogue on the Question of Gender Theory in Education (2019), http://www.educatio.va/content/dam/cec/Documenti/19_0997_INGLESE.pdf.] The Church calls for love and respect for all people.
38. In this guide it outlines both theological and scientific truths about the human person, including that there are two sexes created by God and found in nature, that one cannot separate one’s sex from one’s gender, and that there are biological and unchangeable differences between men and women. Ignoring these truths does not address or help persons who are suffering. […]
46. Science shows that arresting puberty as a gender identity intervention is scientifically dangerous to children. Arresting puberty past its natural onset is therefore ethically, scientifically, and religiously objectionable for CMA members to support. […]
48. These scientific facts are reflected in Christian anthropology, which is ground in biological and medical reality. As one bishop explained in a recent pastoral letter, “We know from biology that a person’s sex is genetically determined at conception and present in every cell of the body. Because the body tells us about ourselves, our biological sex does in fact indicate our inalienable identity as male or female. Thus, so-called transitioning’ might change a person’s appearance and physical traits (hormones, breasts, genitalia, etc.) but does not in fact change the truth of the person’s identity as male or female, a truth reflected in every cell of the body.” “Indeed, no amount of masculinizing’ or ‘feminizing’ hormones or surgery can make a man into a woman, or a woman into a man.” (6) [6: Most Rev. Michael F. Burbidge, Bishop of Arlington, A Catechesis on the Human Person and Gender Ideology, https://www.arlingtondiocese.org/bishop/public-messages/2021/a-catechesis-on-the-human-person-and-gender-ideology/. Of course, at the same time, every “disciple of Christ desires to love all people and to seek their good actively. Denigration or bullying of any person, including those struggling with gender dysphoria, is to be rejected as completely incompatible with the Gospel.” Id.] As a result, the “claim to ‘be transgender’ or the desire to seek ‘transition’ rests on a mistaken view of the human person, rejects the body as a gift from God, and leads to grave harm. To affirm someone in an identity at odds with biological sex or to affirm a person’s desired ‘transition’ is to mislead that person. It involves speaking and interacting with that person in an untruthful manner.” Id.
49. CMA thus urges healthcare professionals to adhere to genetic science and sexual complementarity over ideology in the treatment of gender dysphoria in children. This includes especially avoiding puberty suppression and the use of cross-sex hormones in children with gender dysphoria. One’s sex is not a social construct, but an unchangeable biological reality.
50. In accord with these scientific and religious understandings, CMA and its members believe that healthcare that provides gender-transition procedures and interventions is neither healthful nor caring; it is experimental and dangerous.
51. For CMA and its members, gender-transition procedures and interventions can be harmful, particularly to children, and medical science does not support the provision of such procedures or interventions.
52. CMA and its members thus believe providing or referring patients for the provision of gender identity interventions violates their core beliefs and their oath to “do no harm.”
53. CMA thus opposes pubertal suppression of minors, as well as hormone administration or other surgical interventions for purposes of “choosing” a gender or sex, and it objects to engaging in speech affirming these gender interventions.
54. CMA has adopted an official resolution stating, “the Catholic Medical Association does not support the use of any hormones, hormone blocking agents or surgery in all human persons for the treatment of Gender Dysphoria.”
55. CMA has adopted an official resolution stating, “Catholic Medical Association and its members reject all policies that condition children to accept as normal a life of chemical and surgical impersonation of the opposite sex” as well as “the use of puberty blocking hormones and cross-sex hormones.”
69. The gender identity mandate requires CMA members to engage in various practices to which our members objection on medical and ethical grounds, including the following: […]
m. Saying in their professional opinions that these gender intervention procedures are the standard of care, are safe, are beneficial, are not experimental, or should otherwise be recommended; […]
For ease of reference, the items in this list will be referred to as the “objectionable practices.”
70. The objectionable practices violate the teachings of the Church, and our organization’s members cannot carry them out in good conscience. […]
130. Our members’ sincerely held religious beliefs prohibit them providing, offering, facilitating, or referring for gender transition interventions and also from engaging in or facilitating the objectionable practices. […]
138. CMA’s members are healthcare providers who object on grounds of science and medical ethics, as well as on religious grounds, to providing, offering, participating in, referring for, or paying for the objectionable practices.
###
Attachment: Gender Analysis FLBOM complaint 1 (PDF, 776KB)


{kind=link}
Pingback: Round two: Gender Analysis calls on Florida Boards of Medicine to stop the trans youth care bans and investigate critical irregularities in the rulemaking process | Gender Analysis