
Disclaimer: I am not a medical professional and this is not medical advice.
Previously:
 In trans adolescents, puberty-blocking GnRH agonists to halt the progression of unwanted other-sexed puberty are ideally given at Tanner stage 2 or 3 before those changes can take place, although many youth still do not obtain blockers until Tanner stage 4 or 5 – in effect, transitioning as adults. The accepted wisdom in early transition treatment holds that if blockers are started at stages 2-3, the absence of natal sex hormones means that viable gametes will not develop, and continuation onto cross-sex hormone therapy without interruption means that gametes will never develop, making fertility preservation impossible (Hembree et al., 2017):
In trans adolescents, puberty-blocking GnRH agonists to halt the progression of unwanted other-sexed puberty are ideally given at Tanner stage 2 or 3 before those changes can take place, although many youth still do not obtain blockers until Tanner stage 4 or 5 – in effect, transitioning as adults. The accepted wisdom in early transition treatment holds that if blockers are started at stages 2-3, the absence of natal sex hormones means that viable gametes will not develop, and continuation onto cross-sex hormone therapy without interruption means that gametes will never develop, making fertility preservation impossible (Hembree et al., 2017):
Treating early pubertal youth with GnRH analogs will temporarily impair spermatogenesis and oocyte maturation. Given that an increasing number of transgender youth want to preserve fertility potential, delaying or temporarily discontinuing GnRH analogs to promote gamete maturation is an option. This option is often not preferred, because mature sperm production is associated with later stages of puberty and with the significant development of secondary sex characteristics.
This poses difficulties for trans youth who may wish to have biological children in the future, and this obstacle has been misused by anti-trans advocates to assert that trans youth should therefore experience none of the known benefits of early transition with puberty blockers. However, this issue may not be completely intractable: two cases have been reported of adolescent trans boys, receiving puberty blockers at stage 2, undergoing successful ovarian stimulation and retrieving viable eggs with only a brief interruption before continuing onto testosterone.
What about trans girls and transfeminine adolescents? No such cases of successful fertility preservation had been identified or reported – until last month. Adeleye et al. (2021) describe the case of a trans girl who had been taking puberty blockers since Tanner stage 2 and had continued onto estrogen treatment with no interruption, who sought fertility preservation prior to surgery. Extracted testicular tissue was examined for the presence of any viable sperm, and although no mature sperm were found, late spermatids and early spermatids were identified. These stages, which precede the development of mature sperm, indicate that spermatogenesis was taking place even as the patient’s puberty had remained consistently suppressed and her recorded testosterone levels were continuously low.

Crucially, the authors note that “this cryopreserved specimen has not been assessed for fertility potential”, meaning that it is not yet known whether this is a case of successful fertility preservation. Among adult cis men, in-vitro fertilization and successful pregnancies have been achieved with the use of late spermatids rather than mature sperm (Mansour et al., 2000), and even with the use of early spermatids (Tanaka et al., 2018), although with notably lower success rates.
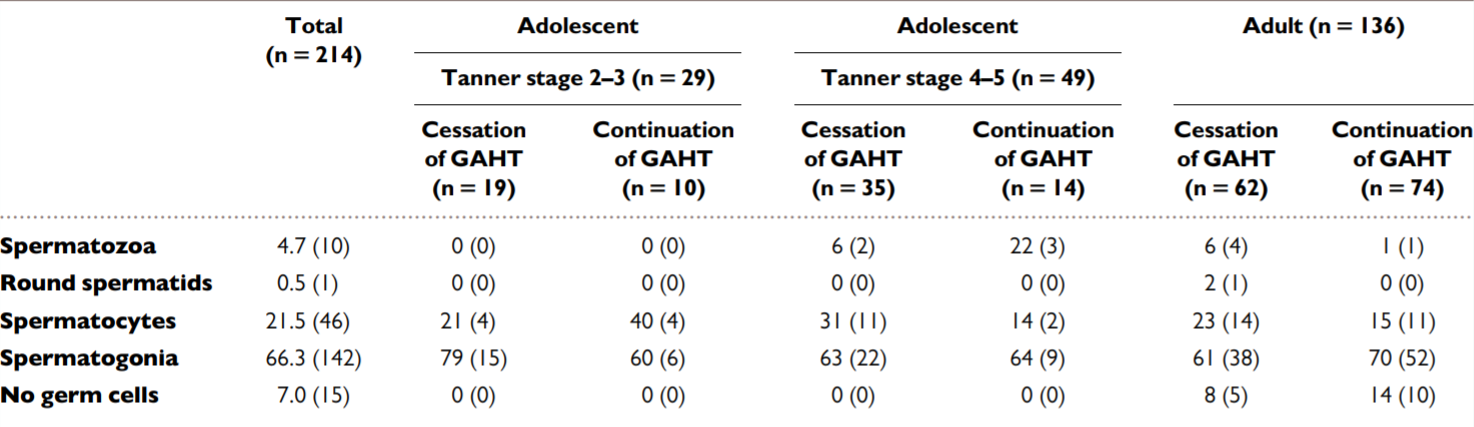
It appears that no cases of the use of late or early spermatids from early-transitioning trans girls for successful fertilization or pregnancy have been reported at present. However, a larger study of this population suggests that this advanced progression of spermatogenesis may be extremely uncommon. This month, de Nie et al. (2021) published their analysis of 29 tissue specimens from trans girls undergoing surgery after starting puberty blockers at Tanner stage 2 or 3. In this group, zero (0) had either mature sperm or spermatids, with most having only early germ cells that cannot be used for fertilization. This included 19 trans girls who had discontinued hormone therapy four weeks before surgery, and 10 who continued taking HRT, suggesting that this period of time was not sufficient for the maturation of sperm or spermatids:
Adeleye et al. similarly point out that when cis boys are given puberty blockers for precocious puberty, 0.7 years to 3 years may be needed after discontinuing puberty blockers before mature sperm begin to appear, meaning that the brief two-week interruption between blockers and HRT as used in the two cases of adolescent trans boys may not be useful for adolescent trans girls.
At present, this recent case appears to indicate that the impossibility of spermatogenesis during early transition is not an absolute rule. However, the larger tissue study contextualizes this as a highly unusual event, and still not an option for almost all early-transitioning trans girls. Adeleye et al. note that this was an “unexpected” finding, and the reason for this extent of spermatogenesis is still unknown in this case given that consistent puberty suppression was confirmed. Other approaches, such as maturing testicular tissue in vitro to produce mature sperm for fertilization, have not yet been carried out successfully in humans, though trans girls may nevertheless have this tissue cryopreserved in anticipation of future developments. Moravek & Obedin-Maliver (2021) have recently called for clinicians to “push boundaries” in the fertility care they provide to trans people; this latest finding may not herald a solved problem, but it does invite us to learn more as we continue working at it. ■


