Her alarmist claims of affirming care for trans youth functioning as anti-gay “conversion therapy” present a scenario wildly at odds with current evidence.
Part 1 — Part 2 — Part 3
Soh continues:
Another phenomenon that points to homophobia as a possible motivation for transitioning is that of rapid-onset gender dysphoria (ROGD), wherein adolescent and college-aged girls suddenly declare to their parents that they want to transition, without any previous signs of being distressed about their birth sex. This desire to transition usually manifests during or after puberty, yet these girls don’t meet any of the diagnostic criteria for gender dysphoria.
This study of “ROGD” did not actually study a single person with this alleged new condition – instead, it relied on anonymous survey responses from parents claiming that their children have experienced this condition, drawn from users of three anti-trans websites that invented the supposed condition in the first place. The distinguishing features of this supposed condition are not really distinguishing at all, with little to separate this from gender dysphoria itself or delineate it as a separate syndrome. When Soh says “these girls” (of whom almost 1 in 5 were actually assigned male, and some were up to age 27), keep in mind that “these girls” were never evaluated in any capacity or even verified to exist at all before they were diagnosed with a condition that may not exist on the basis of anonymous secondhand reports from anti-trans advocates.
It’s notable that earlier in her article, she remarks on gay people who “hid their sexual orientation from anyone outside of the community, and few were openly out to their families”, yet goes on to state that these trans youth “suddenly declare” their transness “without any previous signs”. The explanation for that apparent suddenness seems obvious, but Soh seems to accept without question that this is characteristic of some new phenomenon, as if no parent had ever been surprised before at their child coming out as trans. This is far from the case: existing studies have shown that just as with queer youth, trans youth are also typically aware of their feelings and out to themselves for years before they ever reveal this to anyone else. A parent’s awareness of their child’s gender dysphoria is not at all a reliable proxy for the actual onset of their child’s gender dysphoria.
Soh makes a particularly egregious error in claiming that “these girls don’t meet any of the diagnostic criteria for gender dysphoria”. Even if we were to accept the “ROGD” study as entirely reliable in its methodology and its conclusions, that study says precisely the opposite of what Soh has stated here (Littman, 2018):
It is important to note that none of the AYAs described in this study would have met diagnostic criteria for gender dysphoria in childhood (Table 3). In fact, the vast majority (80.4%) had zero indicators from the DSM-5 diagnostic criteria for childhood gender dysphoria with 12.2% possessing one indicator, 3.5% with two indicators, and 2.4% with three indicators. … Parents responded to the question about which, if any, of the indicators of the DSM criteria for adolescent and adult gender dysphoria their child was experiencing currently. The average number of positive current indicators was 3.5 (range 0–6) and 83.2% of the AYA sample was currently experiencing two or more indicators. Thus, while the focal AYAs did not experience childhood gender dysphoria, the majority of those who were the focus of this study were indeed gender dysphoric at the time of the survey completion.
“These girls” did not meet the DSM-5 diagnostic criteria for childhood gender dysphoria. 83.2% of them did meet the criteria for a diagnosis of adolescent and adult gender dysphoria – yet Soh has incorrectly stated that they do not meet any of the diagnostic criteria. She’s not just using a bad study, she’s misusing a bad study. Did she even read it?
It is especially misleading for her to cite the “ROGD” study in the context of an argument about persistence or desistance of childhood gender dysphoria, given that the study is not about this at all. As stated, the vast majority of “these girls” with ROGD have adolescent and adult gender dysphoria, whereas research on the subject of desistance pertains to whether childhood gender dysphoria will persist and become adolescent and adult gender dysphoria. It says nothing about whether those who already have adolescent and adult gender dysphoria will continue to have it – desistance research is simply not applicable here. Perhaps the closest thing to evidence regarding “desistance” in adolescent and adult gender dysphoria would be the finding that about 2% of adults who transition will regret doing so (Dhejne et al., 2014), or the report from the Royal Children’s Hospital in Australia finding that 4% of adolescents diagnosed with gender dysphoria and referred for treatment with puberty blockers were no longer gender-dysphoric in late adolescence. Alternately, Soh could have referred to the “ROGD” study itself:
At the end of the timeframe, 83.2% of the AYAs were still transgender-identified, 5.5% were not still transgender-identified (desisted), 2.7% seemed to be backing away from transgender-identification, and 8.6% of the parents did not know if their child was still identifying as transgender.
None of this supports the contention that a majority of these youth will grow up to be cisgender gay adults. While that argument may be made regarding gender-dysphoric children (even as she uses it to draw entirely inaccurate conclusions based on her own ignorance of treatment protocols), it certainly does not hold up in the case of gender-dysphoric adolescents. Soh is talking about two distinct populations with distinct developmental trajectories and patterns of outcomes, yet treats them as though they are essentially interchangeable.
Citing the alleged “ROGD” phenomenon to support this narrative of homophobia-driven transition is a comically ineffective choice of argument, and one that totally backfires. Soh claims:
A study published last month on ROGD—one that gained widespread media attention for infuriating transgender activists—found that a large proportion of these girls had come out as lesbian or bisexual prior to coming out as transgender.
Let’s look at just what that study found about the sexual orientation of youth whose parents were surveyed:
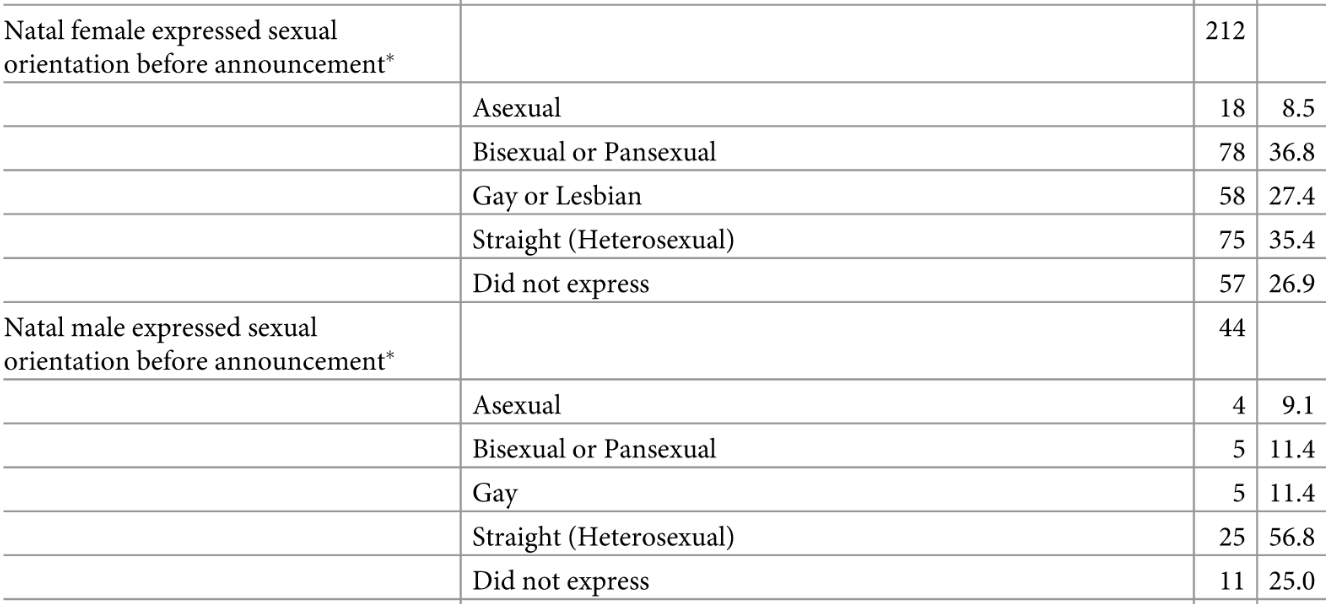
Littman (2018), fig. 2 (respondents may have selected more than one answer)
Of the assigned-female youth, 27.4% were reported to have been gay or lesbian (attracted to women) before coming out, 36.8% were bisexual or pansexual, and 35.4% were straight (attracted to men). Assuming no overlap due to multiple answers, this would be a total of 64.2% whose sexual orientation included same-sex attraction. (A further 8.5% were reportedly asexual, while another 26.9% “did not express” a sexual orientation.) Now suppose every one of these youth were to transition and adopt an identity as trans men, with an accompanying change in how their sexual orientation is perceived and labeled due to presenting and identifying as men rather than women. Were that to happen, 35.4% of these men would be gay (attracted to men), 36.8% would be bisexual or pansexual, and 27.4% would be straight (attracted to women), for a total of 72.2% whose sexual orientation included same-sex attraction. This would result in more of this group being labeled as having a gay sexual orientation, and fewer having a straight sexual orientation.
And for assigned-male youth included in the study? 11.4% were reported to be gay (attracted to men), 11.4% were bisexual or pansexual, and 56.8% were straight (attracted to women). If they were all to adopt identities as trans women, 56.8% would be lesbian (attracted to women), 11.4% would be bisexual or pansexual, and 11.4% would be straight. Once again, more would be labeled as lesbian, and fewer as straight.
Based on the distribution of sexual orientation in the sample of youth who are alleged to have “ROGD”, a condition of universal transition would result in far more of them being perceived as gay compared to a condition of universal non-transition. In what way could transition then be said to serve as some kind of social escape hatch from being perceived as gay? If such a motivation were at work here – and there is no evidence of this – if anything, it would indicate that transition serves as a social escape hatch from being perceived as straight. Exactly what kind of anti-gay “conversion therapy” is that? Did Debra Soh, who “holds a Ph.D. in sexual neuroscience research from York University and writes about the science and politics of sex”, read this study?
Next: Societal homophobia, family transphobia, and the era of trans ignorance.


 Earlier this year, I reviewed the occurrence of meningioma, a typically benign brain tumor, among trans women using the antiandrogen cyproterone acetate (CPA). Meningiomas, the most common type of brain tumor (Saraf, McCarthy & Villano, 2011), develop in the membranes surrounding the brain and can produce symptoms such as headaches, seizures, muscle weakness, vision loss, and memory loss, while others are asymptomatic and may only be found incidentally in medical imaging (Spasic et al., 2016). About 70-88% of meningiomas express progesterone receptors (Blitshteyn, Crook, & Jaeckle, 2008; Korhonen et al., 2006), suggesting that the progestogenic action of CPA may encourage growth of these tumors. Use of CPA in high doses – 50 mg/day or more – has been found to be associated with an increased incidence of meningioma in cis women and cis men (Gil et al., 2011). Continue reading
Earlier this year, I reviewed the occurrence of meningioma, a typically benign brain tumor, among trans women using the antiandrogen cyproterone acetate (CPA). Meningiomas, the most common type of brain tumor (Saraf, McCarthy & Villano, 2011), develop in the membranes surrounding the brain and can produce symptoms such as headaches, seizures, muscle weakness, vision loss, and memory loss, while others are asymptomatic and may only be found incidentally in medical imaging (Spasic et al., 2016). About 70-88% of meningiomas express progesterone receptors (Blitshteyn, Crook, & Jaeckle, 2008; Korhonen et al., 2006), suggesting that the progestogenic action of CPA may encourage growth of these tumors. Use of CPA in high doses – 50 mg/day or more – has been found to be associated with an increased incidence of meningioma in cis women and cis men (Gil et al., 2011). Continue reading 
